

A new standard of care for the management of peritoneal surface malignancy
- PMID: 21505593
- PMCID: PMC3070715
- DOI: 10.3747/co.v18i2.663
A new standard of care for the management of peritoneal surface malignancy
Abstract
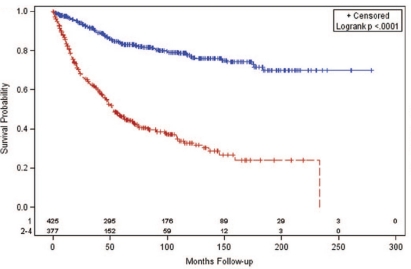
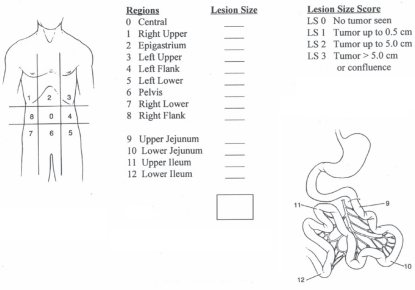
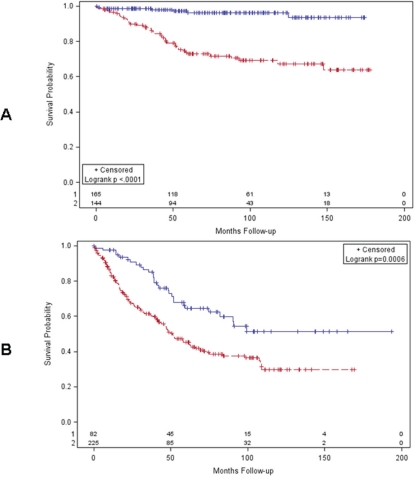
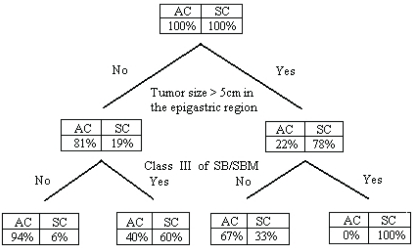
Cancer dissemination to peritoneal surfaces was, in the past, a lethal condition with a limited survival. Clinical and pharmacologic research have shown that options for both treatment and prevention are now reality. The diseases most commonly treated include peritoneal dissemination from appendiceal malignancy, colorectal malignancy, and peritoneal mesothelioma. Selection factors are important to minimize the number of treated patients who will experience short-term benefit. Treatments involve cytoreductive surgery and perioperative chemotherapy. The intraperitoneal chemotherapy in the operating room is used with heat. Although this combined approach has been criticized, the informed oncologist will seek to identify those patients that may benefit from this more optimistic concept of peritoneal dissemination of cancer.
Keywords: Cytoreductive surgery; appendiceal cancer; carcinomatosis; colorectal cancer; hipec; hyperthermic intraperitoneal chemotherapy; mitomycin C; peritoneal mesothelioma; pseudomyxoma peritonei.
Figures
References
-
- West NP, Hohenberger W, Weber K, Perrakis A, Finan PJ, Quirke P. Complete mesocolic excision with central vascular ligation produces an oncologically superior specimen compared with standard surgery for carcinoma of the colon. J Clin Oncol. 2010;28:272–8. doi: 10.1200/JCO.2009.24.1448. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
