

Indications of Th1 and Th17 responses in cerebrospinal fluid from patients with Lyme neuroborreliosis: a large retrospective study
- PMID: 21507218
- PMCID: PMC3108302
- DOI: 10.1186/1742-2094-8-36
Indications of Th1 and Th17 responses in cerebrospinal fluid from patients with Lyme neuroborreliosis: a large retrospective study
Abstract
Background: Previous studies indicate that successful resolution of Lyme neuroborreliosis (NB) is associated with a strong T helper (Th) 1-type cytokine response in the cerebrospinal fluid (CSF) followed by a down-regulating Th2 response, whereas the role of the recently discovered Th17 cytokine response is unknown.
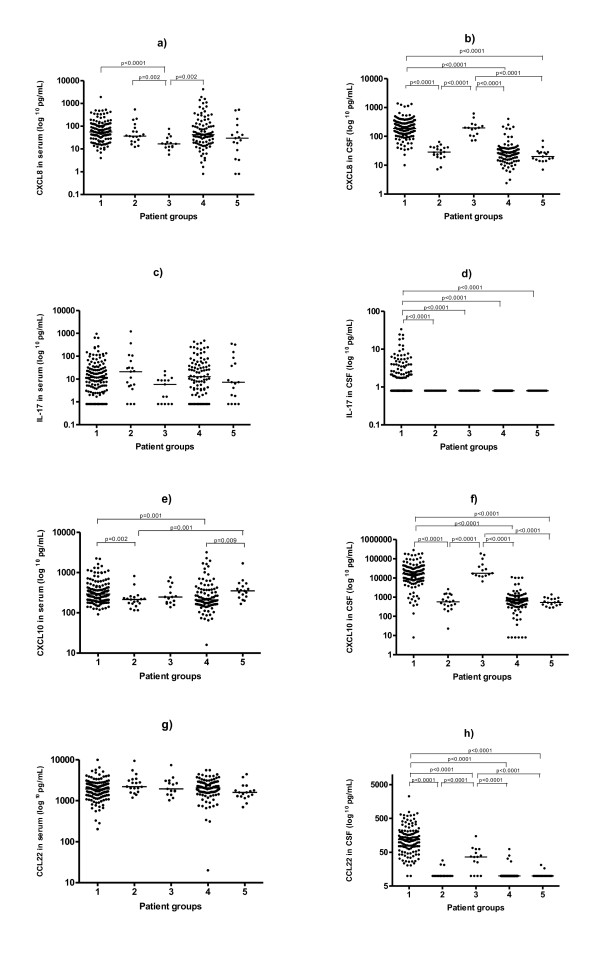
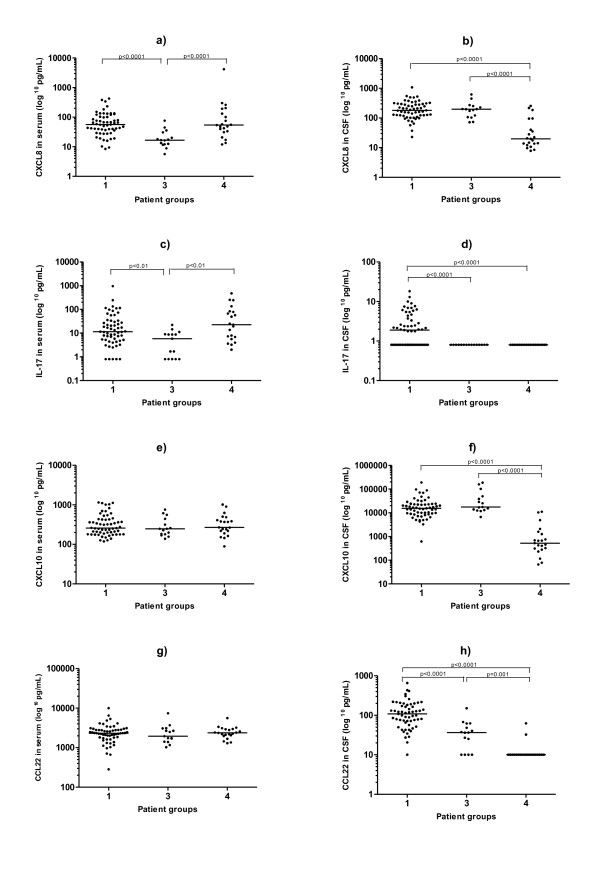
Methods: To investigate the relative contribution of different Th associated cytokine/chemokine responses, we used a multiple bead array to measure the levels of CXCL10 (Th1 marker), CCL22 (Th2 marker), IL-17 (Th17 marker) and CXCL8 (general inflammation marker), in serum and in CSF from untreated patients with confirmed NB (n = 133), and non-NB patients (n = 96), and related the findings to clinical data. Samples from patients with possible early NB (n = 15) and possible late NB (n = 19) were also analysed, as well as samples from an additional control group with orthopaedic patients (n = 17), where CSF was obtained at spinal anaesthesia.
Results: The most prominent differences across groups were found in the CSF. IL-17 was elevated in CSF in 49% of the patients with confirmed NB, but was not detectable in the other groups. Patients with confirmed NB and possible early NB had significantly higher CSF levels of CXCL10, CCL22 and CXCL8 compared to both the non-NB group and the control group (p < 0.0001 for all comparisons). Patients in the early NB group, showing a short duration of symptoms, had lower CCL22 levels in CSF than did the confirmed NB group (p < 0.0001). Furthermore, patients within the confirmed NB group showing a duration of symptoms <2 weeks, tended to have lower CCL22 levels in CSF than did those with longer symptom duration (p = 0.023). Cytokine/chemokine levels were not correlated with clinical parameters or to levels of anti-Borrelia-antibodies.
Conclusion: Our results support the notion that early NB is dominated by a Th1-type response, eventually accompanied by a Th2 response. Interestingly, IL-17 was increased exclusively in CSF from patients with confirmed NB, suggesting a hitherto unknown role for Th17 in NB. However, for conclusive evidence, future prospective studies are needed.
Figures
Similar articles
-
Intrathecal Th17- and B cell-associated cytokine and chemokine responses in relation to clinical outcome in Lyme neuroborreliosis: a large retrospective study.J Neuroinflammation. 2017 Feb 1;14(1):27. doi: 10.1186/s12974-017-0789-6. J Neuroinflammation. 2017. PMID: 28148307 Free PMC article.
-
The chemotactic cytokines in the cerebrospinal fluid of patients with neuroborreliosis.Cytokine. 2021 Jun;142:155490. doi: 10.1016/j.cyto.2021.155490. Epub 2021 Mar 18. Cytokine. 2021. PMID: 33744829
-
Evaluation of CXCL8, CXCL10, CXCL11, CXCL12 and CXCL13 in serum and cerebrospinal fluid of patients with neuroborreliosis.Immunol Lett. 2014 Jan-Feb;157(1-2):45-50. doi: 10.1016/j.imlet.2013.11.002. Epub 2013 Nov 12. Immunol Lett. 2014. PMID: 24239846
-
Cerebrospinal fluid cytokines in Lyme neuroborreliosis.J Neuroinflammation. 2016 Oct 18;13(1):273. doi: 10.1186/s12974-016-0745-x. J Neuroinflammation. 2016. PMID: 27756335 Free PMC article.
-
Up-regulation of Borrelia-specific IL-4- and IFN-gamma-secreting cells in cerebrospinal fluid from children with Lyme neuroborreliosis.Int Immunol. 2005 Oct;17(10):1283-91. doi: 10.1093/intimm/dxh304. Int Immunol. 2005. PMID: 16176932
Cited by
-
The multifaceted responses of primary human astrocytes and brain microvascular endothelial cells to the Lyme disease spirochete, Borrelia burgdorferi.ASN Neuro. 2013 Aug 16;5(3):221-9. doi: 10.1042/AN20130010. ASN Neuro. 2013. PMID: 23883071 Free PMC article.
-
Infection of Interleukin 17 Receptor A-Deficient C3H Mice with Borrelia burgdorferi Does Not Affect Their Development of Lyme Arthritis and Carditis.Infect Immun. 2015 Jul;83(7):2882-8. doi: 10.1128/IAI.00533-15. Epub 2015 May 4. Infect Immun. 2015. PMID: 25939508 Free PMC article.
-
Autophagy suppresses host adaptive immune responses toward Borrelia burgdorferi.J Leukoc Biol. 2016 Sep;100(3):589-98. doi: 10.1189/jlb.4A0715-331R. Epub 2016 Apr 21. J Leukoc Biol. 2016. PMID: 27101991 Free PMC article.
-
The Potential of Omics Technologies in Lyme Disease Biomarker Discovery and Early Detection.Infect Dis Ther. 2017 Mar;6(1):85-102. doi: 10.1007/s40121-016-0138-6. Epub 2016 Nov 29. Infect Dis Ther. 2017. PMID: 27900646 Free PMC article. Review.
-
ssICAM-1, IL-21 and IL-23 in patients with tick borne encephalitis and neuroborreliosis.Cytokine. 2012 Nov;60(2):468-72. doi: 10.1016/j.cyto.2012.05.007. Epub 2012 Jun 15. Cytokine. 2012. PMID: 22705151 Free PMC article.
References
-
- Weber K. Aspects of Lyme borreliosis in Europe. Eur J Clin Microbiol Infect Dis. 2001;20:6–13. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
