

A comparison of four fibrosis indexes in chronic HCV: development of new fibrosis-cirrhosis index (FCI)
- PMID: 21507271
- PMCID: PMC3098184
- DOI: 10.1186/1471-230X-11-44
A comparison of four fibrosis indexes in chronic HCV: development of new fibrosis-cirrhosis index (FCI)
Abstract
Background: Hepatitis C can lead to liver fibrosis and cirrhosis. We compared readily available non-invasive fibrosis indexes for the fibrosis progression discrimination to find a better combination of existing non-invasive markers.
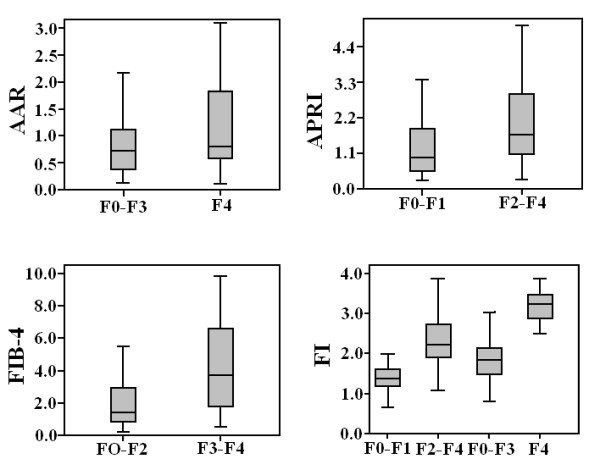
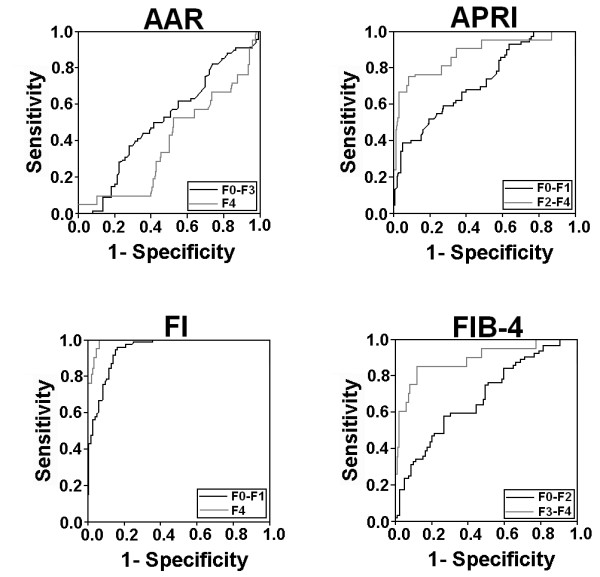
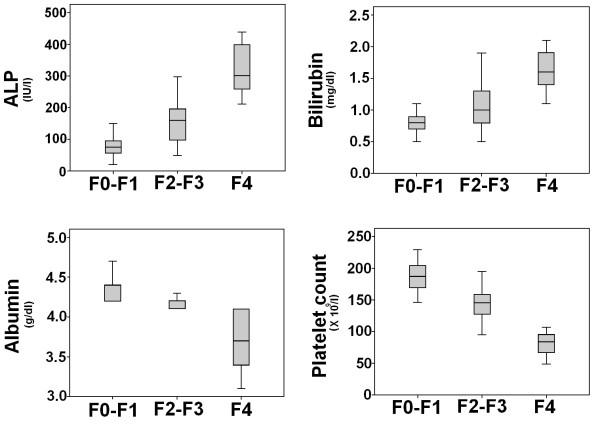
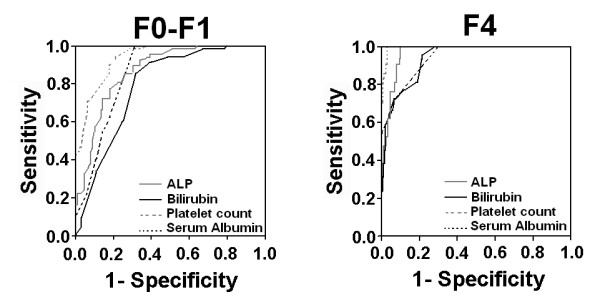
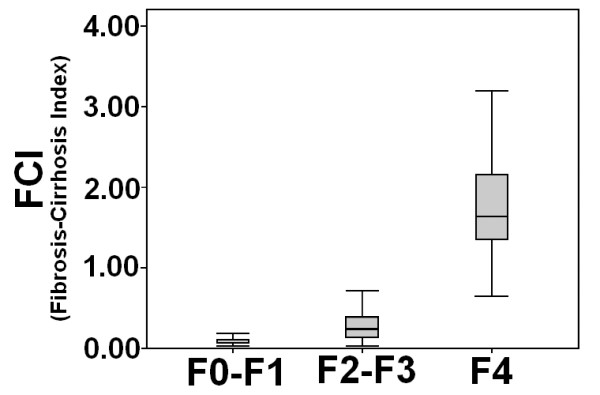
Methods: We studied 157 HCV infected patients who underwent liver biopsy. In order to differentiate HCV fibrosis progression, readily available AAR, APRI, FI and FIB-4 serum indexes were tested in the patients. We derived a new fibrosis-cirrhosis index (FCI) comprised of ALP, bilirubin, serum albumin and platelet count. FCI = [(ALP × Bilirubin) / (Albumin × Platelet count)].
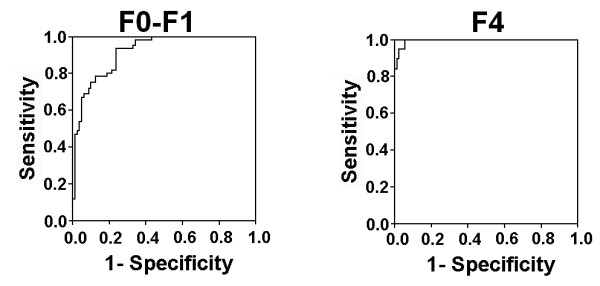
Results: Already established serum indexes AAR, APRI, FI and FIB-4 were able to stage liver fibrosis with correlation coefficient indexes 0.130, 0.444, 0.578 and 0.494, respectively. Our new fibrosis cirrhosis index FCI significantly correlated with the histological fibrosis stages F0-F1, F2-F3 and F4 (r = 0.818, p < 0.05) with AUROCs 0.932 and 0.996, respectively. The sensitivity and PPV of FCI at a cutoff value < 0.130 for predicting fibrosis stage F0-F1 was 81% and 82%, respectively with AUROC 0.932. Corresponding value of FCI at a cutoff value ≥1.25 for the prediction of cirrhosis was 86% and 100%.
Conclusions: The fibrosis-cirrhosis index (FCI) accurately predicted fibrosis stages in HCV infected patients and seems more efficient than frequently used serum indexes.
Figures
References
-
- Giannini C, Brechot C. Hepatitis C virus biology. J Virology. 2003;10:S27–S38. - PubMed
-
- Raja NS, Janjua KA. Epidemiology of hepatitis C virus infection in Pakistan. J Microbiol Immunol Infect. 2008;41:4–8. - PubMed
-
- EL-Serag HB. Hepatocellular carcinoma and hepatitis C in the United States. Hepatology. 2002;36:S74–S83. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
