

The postoperative basal cortisol and CRH tests for prediction of long-term remission from Cushing's disease after transsphenoidal surgery
- PMID: 21508126
- PMCID: PMC3135190
- DOI: 10.1210/jc.2011-0456
The postoperative basal cortisol and CRH tests for prediction of long-term remission from Cushing's disease after transsphenoidal surgery
Abstract
Context: Selective adenomectomy via transsphenoidal surgery induces remission of Cushing's disease (CD) in most patients. Although an undetectable postoperative serum cortisol (<2 μg/dl) has been advocated as an index of remission, there is no consensus on predictors of recurrence.
Objective: We hypothesized that patients with subnormal cortisol (2-4.9 μg/dl) might achieve long-term remission and that postoperative responses to CRH might predict recurrence.
Design, setting, and participants: We prospectively studied CD patients with initial remission after adenomectomy or hemihypophysectomy (n = 14). Long-term recurrence (n = 39) or remission (n = 293) was assigned by laboratory results, glucocorticoid dependence, or patient survey at a mean of 10.6 yr after surgery.
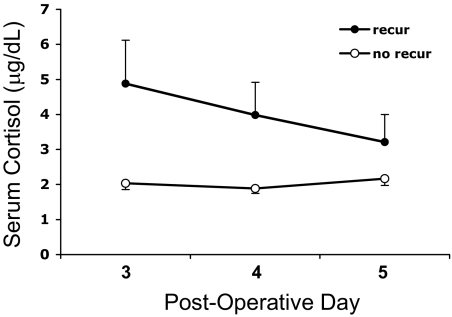
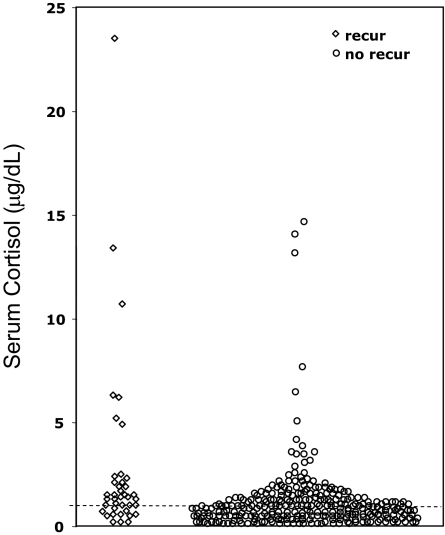
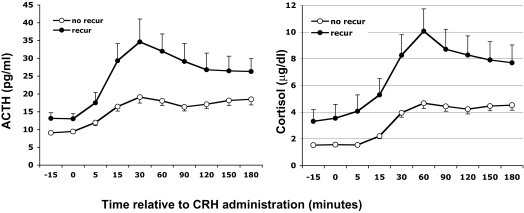
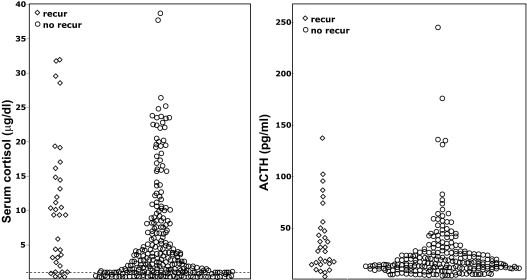
Intervention and main outcome measures: Postoperatively, morning cortisol was measured on d 3-5, and cortisol and ACTH responses to ovine CRH were assessed around d 10.
Results: Follow-up duration was median 11 yr (range 1-22.8 yr). Fewer patients achieved a cortisol nadir below 2 μg/dl (87%) than below 5 μg/dl (98%), yet recurrence rates were similar (<2 μg/dl, 9.5%; <5 μg/dl, 10.4%; 2-4.9 μg/dl, 20%; not significant). CRH-stimulated cortisol (P < 0.002) and ACTH (P = 0.04) values were higher for the recurrence than the remission group. However, no basal or stimulated ACTH or serum or urine cortisol cutoff value predicted all who later recurred.
Conclusions: A postoperative cortisol below 2 μg/dl predicts long-term remission after transsphenoidal surgery in CD. Remission in those with intermediate d 3-5 postoperative cortisol values (2-4.9 μg/dl) suggests that these patients do not require immediate reoperation. However, because no single cortisol cutoff value excludes all patients with recurrence, all require long-term clinical follow-up.
Figures
Similar articles
-
Dynamics of postoperative serum cortisol after transsphenoidal surgery for Cushing's disease: implications for immediate reoperation and remission.J Neurosurg. 2018 Nov 1;129(5):1268-1277. doi: 10.3171/2017.6.JNS17635. Epub 2017 Dec 22. J Neurosurg. 2018. PMID: 29271716
-
Remission rate after transsphenoidal surgery in patients with pathologically confirmed Cushing's disease, the role of cortisol, ACTH assessment and immediate reoperation: a large single center experience.Pituitary. 2013 Dec;16(4):452-8. doi: 10.1007/s11102-012-0455-z. Pituitary. 2013. PMID: 23242860
-
Biochemical predictors of outcome of pituitary surgery for Cushing's disease.Neuroendocrinology. 2010;91(2):169-78. doi: 10.1159/000258677. Epub 2009 Nov 12. Neuroendocrinology. 2010. PMID: 19907141
-
Negative surgical exploration in patients with Cushing's disease: benefit of two-thirds gland resection on remission rate and a review of the literature.J Neurosurg. 2018 Nov 1;129(5):1260-1267. doi: 10.3171/2017.5.JNS162901. J Neurosurg. 2018. PMID: 29219752 Review.
-
Criteria of cure and remission in Cushing's disease: an update.Arq Bras Endocrinol Metabol. 2007 Nov;51(8):1362-72. doi: 10.1590/s0004-27302007000800023. Arq Bras Endocrinol Metabol. 2007. PMID: 18209875 Review.
Cited by
-
Cushing's syndrome: epidemiology and developments in disease management.Clin Epidemiol. 2015 Apr 17;7:281-93. doi: 10.2147/CLEP.S44336. eCollection 2015. Clin Epidemiol. 2015. PMID: 25945066 Free PMC article. Review.
-
Hormonal aggressiveness according to the expression of cellular markers in corticotroph adenomas.Endocrine. 2019 Apr;64(1):147-156. doi: 10.1007/s12020-018-1815-x. Epub 2018 Nov 24. Endocrine. 2019. PMID: 30474823
-
A Comprehensive Approach to Predicting the Outcomes of Transsphenoidal Endoscopic Adenomectomy in Patients with Cushing's Disease.J Pers Med. 2022 May 16;12(5):798. doi: 10.3390/jpm12050798. J Pers Med. 2022. PMID: 35629220 Free PMC article.
-
Diurnal Range and Intra-patient Variability of ACTH Is Restored With Remission in Cushing's Disease.J Clin Endocrinol Metab. 2023 Oct 18;108(11):2812-2820. doi: 10.1210/clinem/dgad309. J Clin Endocrinol Metab. 2023. PMID: 37261392 Free PMC article.
-
Quality of life and other outcomes in children treated for Cushing syndrome.J Clin Endocrinol Metab. 2013 Jul;98(7):2667-78. doi: 10.1210/jc.2013-1123. Epub 2013 May 2. J Clin Endocrinol Metab. 2013. PMID: 23640970 Free PMC article. Review.
References
-
- Arnaldi G, Angeli A, Atkinson AB, Bertagna X, Cavagnini F, Chrousos GP, Fava GA, Findling JW, Gaillard RC, Grossman AB, Kola B, Lacroix A, Mancini T, Mantero F, Newell-Price J, Nieman LK, Sonino N, Vance ML, Giustina A, Boscaro M. 2003. Diagnosis and complications of Cushing's syndrome: a consensus statement. J Clin Endocrinol Metab 88:5593–5602 - PubMed
-
- Hammer GD, Tyrrell JB, Lamborn KR, Applebury CB, Hannegan ET, Bell S, Rahl R, Lu A, Wilson CB. 2004. Transsphenoidal microsurgery for Cushing's disease: initial outcome and long-term results. J Clin Endocrinol Metab 89:6348–6357 - PubMed
-
- Swearingen B, Biller BM, Barker FG, 2nd, Katznelson L, Grinspoon S, Klibanski A, Zervas NT. 1999. Long-term mortality after transsphenoidal surgery for Cushing disease. Ann Intern Med 130:821–824 - PubMed
-
- Nieman LK, Oldfield EH, Wesley R, Chrousos GP, Loriaux DL, Cutler GB., Jr 1993. A simplified morning ovine corticotropin-releasing hormone stimulation test for the differential diagnosis of adrenocorticotropin-dependent Cushing's syndrome. J Clin Endocrinol Metab 77:1308–1312 - PubMed
-
- Oldfield EH, Doppman JL, Nieman LK, Chrousos GP, Miller DL, Katz DA, Cutler GB, Jr, Loriaux DL. 1991. Petrosal sinus sampling with and without corticotropin-releasing hormone for the differential diagnosis of Cushing's syndrome. N Engl J Med 325:897–905 - PubMed
