

Inflammatory profile and response to anti-tumor necrosis factor therapy in patients with chronic pulmonary sarcoidosis
- PMID: 21508170
- PMCID: PMC3122612
- DOI: 10.1128/CVI.00337-10
Inflammatory profile and response to anti-tumor necrosis factor therapy in patients with chronic pulmonary sarcoidosis
Abstract
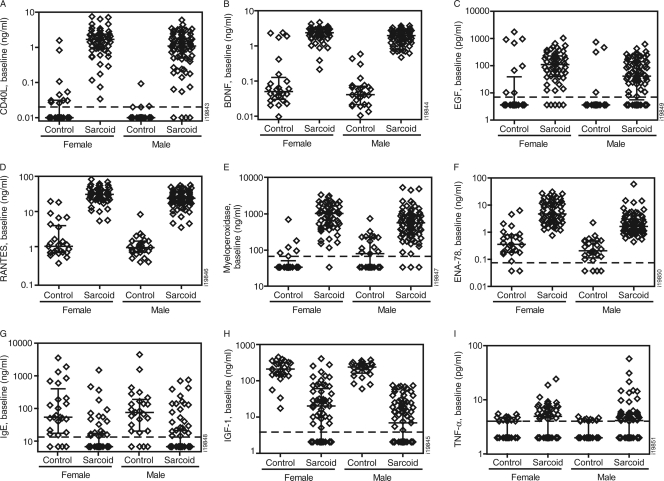
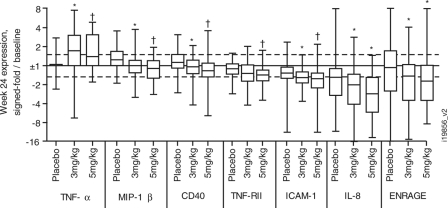
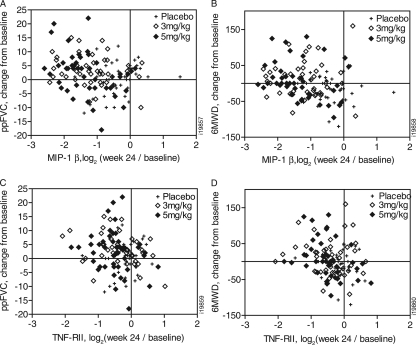
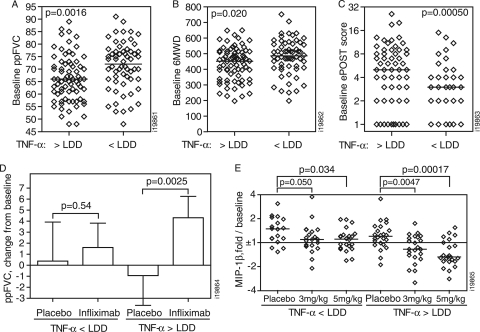
Sarcoidosis is an inflammatory, granulomatous disease of unknown etiology that most commonly afflicts the lungs. Despite aggressive immunosuppressive therapies, many sarcoidosis patients still chronically present significant symptoms. Infliximab, a therapeutic tumor necrosis factor alpha (TNF-α) monoclonal antibody (MAb), produced a small but significant improvement in forced vital capacity (FVC) in sarcoidosis patients in a double-blind, placebo-controlled, phase II clinical trial. In the current study, serum samples from this clinical trial were assessed to evaluate the underlying hypothesis that treatment with infliximab would reduce systemic inflammation associated with sarcoidosis, correlating with the extent of clinical response. A 92-analyte multiplex panel was used to assess the expression of serum proteins in 134 sarcoidosis patients compared with sera from 50 healthy controls. A strong systemic inflammatory profile was associated with sarcoidosis, with 29 analytes significantly elevated in sarcoidosis (false-discovery rate, <0.05 and >50% higher than controls). The associated analytes included chemokines, neutrophil-associated proteins, acute-phase proteins, and metabolism-associated proteins. This profile was evident despite patients receiving corticosteroids and immunosuppressive therapies. Following infliximab treatment, sarcoidosis patients expressing the highest levels of TNF-α, who had more severe disease, had the greatest improvement in FVC and reduction in serum levels of the inflammatory proteins MIP-1β and TNF-RII. This study supports the need for further exploration of anti-TNF therapy for chronic sarcoidosis patients, particularly for those expressing the highest serum levels of TNF-α.
Figures
Similar articles
-
Infliximab therapy in patients with chronic sarcoidosis and pulmonary involvement.Am J Respir Crit Care Med. 2006 Oct 1;174(7):795-802. doi: 10.1164/rccm.200603-402OC. Epub 2006 Jul 13. Am J Respir Crit Care Med. 2006. PMID: 16840744 Clinical Trial.
-
Systemic inflammatory profile and response to anti-tumor necrosis factor therapy in chronic obstructive pulmonary disease.Respir Res. 2012 Feb 2;13(1):12. doi: 10.1186/1465-9921-13-12. Respir Res. 2012. PMID: 22300528 Free PMC article. Clinical Trial.
-
Infliximab for treating sarcoidosis patients, Portuguese experience.Rev Port Pneumol. 2011 Mar-Apr;17(2):85-93. Rev Port Pneumol. 2011. PMID: 21477572 English, Portuguese.
-
Pulmonary sarcoidosis.Clin Chest Med. 2004 Sep;25(3):521-30, vi. doi: 10.1016/j.ccm.2004.04.006. Clin Chest Med. 2004. PMID: 15331189 Review.
-
Tumour necrosis factor in sarcoidosis and its potential for targeted therapy.BioDrugs. 2003;17(6):425-31. doi: 10.2165/00063030-200317060-00005. BioDrugs. 2003. PMID: 14614765 Review.
Cited by
-
Treatment of Sarcoidosis: A Multidisciplinary Approach.Front Immunol. 2020 Nov 19;11:545413. doi: 10.3389/fimmu.2020.545413. eCollection 2020. Front Immunol. 2020. PMID: 33329511 Free PMC article. Review.
-
Adalimumab for refractory pulmonary sarcoidosis.Ir J Med Sci. 2016 Nov;185(4):969-971. doi: 10.1007/s11845-015-1363-9. Epub 2015 Oct 1. Ir J Med Sci. 2016. PMID: 26428728 Review.
-
Lymphopenia and high Ki-67 expression in peripheral blood CD4+ and CD8+ T cells associate with progressive sarcoidosis.BMJ Open Respir Res. 2023 Dec 14;10(1):e001551. doi: 10.1136/bmjresp-2022-001551. BMJ Open Respir Res. 2023. PMID: 38097354 Free PMC article.
-
Sarcoidosis: Causes, Diagnosis, Clinical Features, and Treatments.J Clin Med. 2020 Apr 10;9(4):1081. doi: 10.3390/jcm9041081. J Clin Med. 2020. PMID: 32290254 Free PMC article. Review.
-
Efficacy and safety of infliximab therapy in refractory upper respiratory tract sarcoidosis: experience from the STAT registry.Sarcoidosis Vasc Diffuse Lung Dis. 2017;34(4):343-351. doi: 10.36141/svdld.v34i4.5817. Epub 2017 Apr 28. Sarcoidosis Vasc Diffuse Lung Dis. 2017. PMID: 32476867 Free PMC article.
References
-
- . 1999. Statement on sarcoidosis. Joint statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, February 1999. Am. J. Respir. Crit. Care Med. 160:736–755 - PubMed
-
- Baughman R. P., et al. 2006. Infliximab therapy in patients with chronic sarcoidosis and pulmonary involvement. Am. J. Respir. Crit. Care Med. 174:795–802 - PubMed
-
- Baughman R. P., Lower E. E., Drent M. 2008. Inhibitors of tumor necrosis factor (TNF) in sarcoidosis: who, what, and how to use them. Sarcoidosis Vasc. Diffuse Lung Dis. 25:76–89 - PubMed
-
- Boots A. W., et al. 2009. Antioxidant status associated with inflammation in sarcoidosis: a potential role for antioxidants. Respir. Med. 103:364–372 - PubMed
-
- Capelli A., Di Stefano A., Lusuardi M., Gnemmi I., Donner C. F. 2002. Increased macrophage inflammatory protein-1alpha and macrophage inflammatory protein-1beta levels in bronchoalveolar lavage fluid of patients affected by different stages of pulmonary sarcoidosis. Am. J. Respir. Crit. Care Med. 165:236–241 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
