

The Clinical Significance of CD4 Counts in Asian and Caucasian HIV-Infected Populations: Results from TAHOD and AHOD
- PMID: 21508296
- PMCID: PMC3337854
- DOI: 10.1177/1545109711402213
The Clinical Significance of CD4 Counts in Asian and Caucasian HIV-Infected Populations: Results from TAHOD and AHOD
Abstract
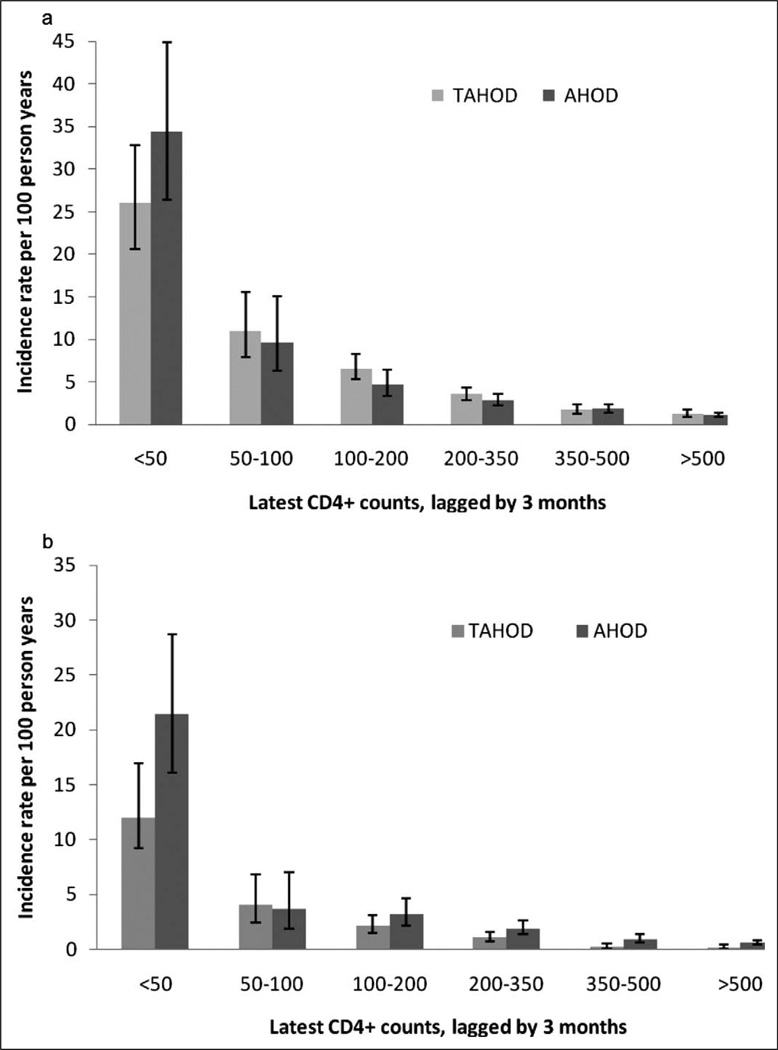
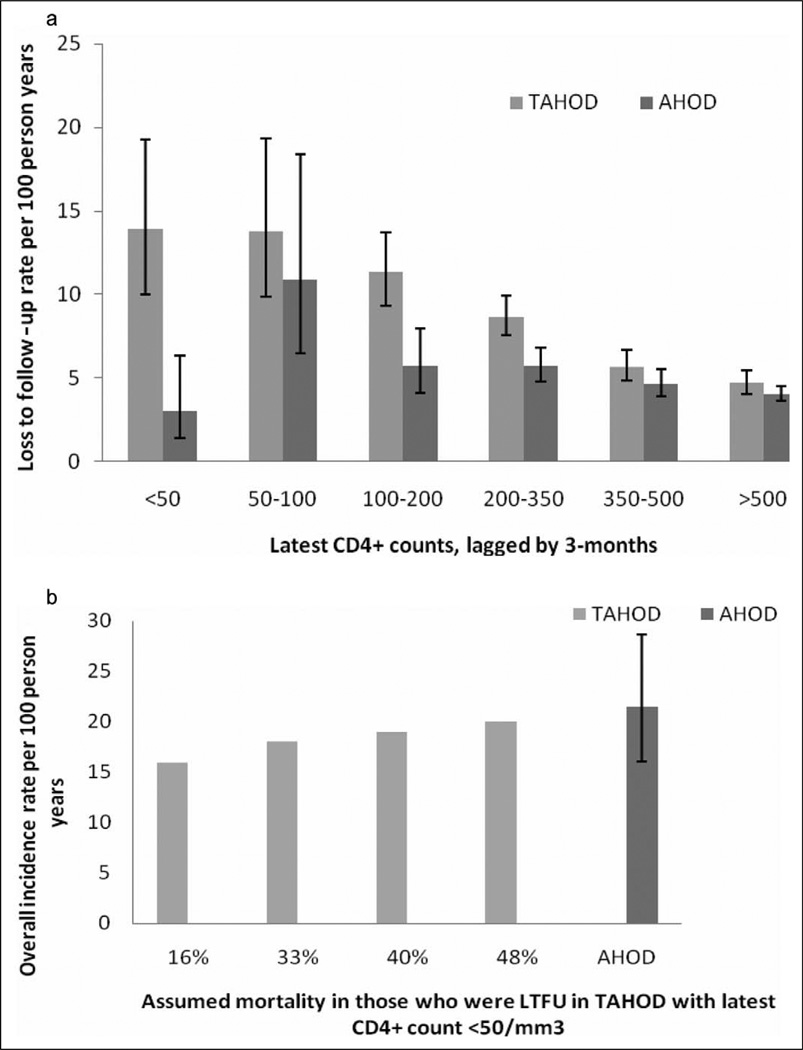
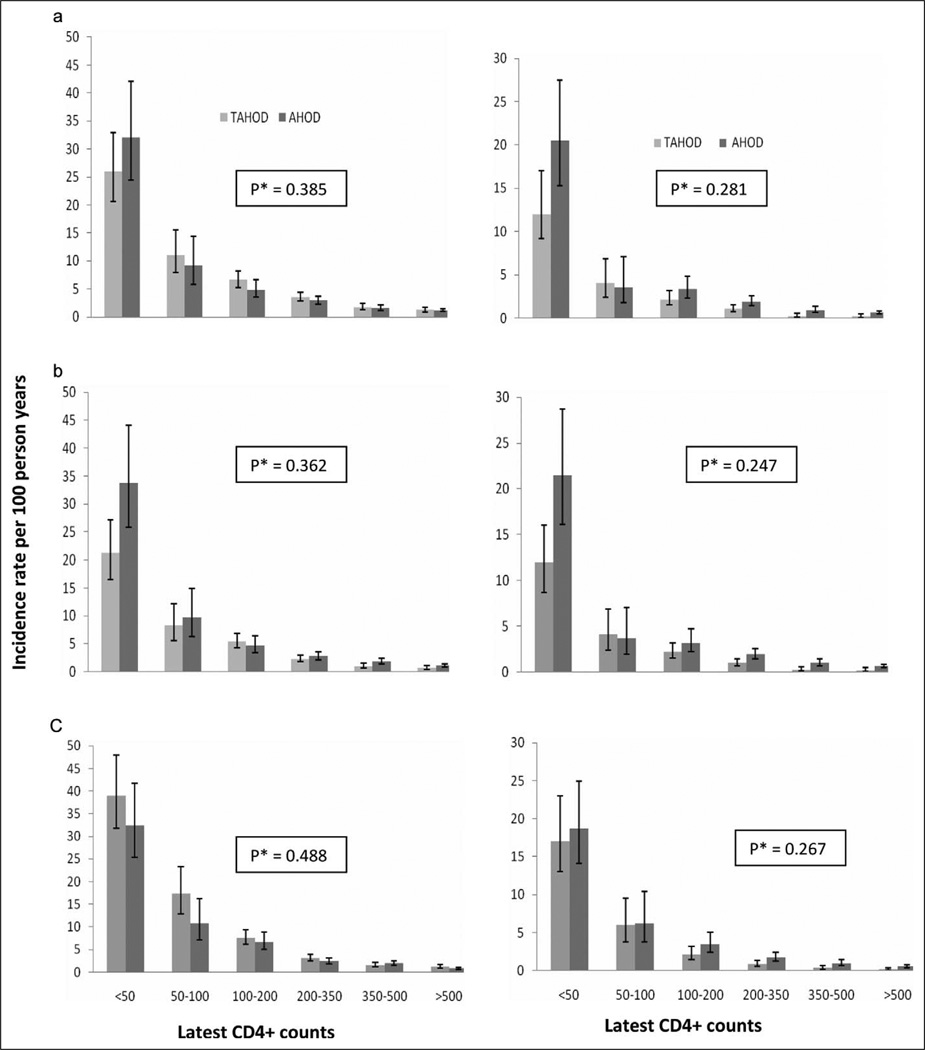
The significance of interethnic variation in CD4 counts between Asian and Caucasian populations is not known. Patients on combination antiretroviral therapy from Treat Asia and Australian HIV Observational Databases (TAHOD, predominantly Asian, n = 3356; and AHOD, predominantly Caucasian, n = 2312, respectively) were followed for 23 144 person-years for AIDS/death and all-cause mortality endpoints. We calculated incidence-rates and used adjusted Cox regression to test for the interaction between cohort (TAHOD/AHOD) and time-updated CD4 count category (lagged by 3 months) for each of the endpoints. There were 382 AIDS/death events in TAHOD (rate: 4.06, 95%CI: 3.68-4.50) and 305 in AHOD (rate: 2.39, 95%CI: 2.13-2.67), per 100 person-years. At any given CD4 count category, the incidence-rates of endpoints were found to be similar between TAHOD and AHOD (in the adjusted models, P > .05 for the interaction term between cohort type and latest CD4 counts). At any given CD4 count, risk of AIDS or death was not found to vary by ethnicity, suggesting that the CD4 count thresholds for predicting outcomes defined in Caucasian populations may be equally valid in Asian populations.
Conflict of interest statement
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
Figures
Similar articles
-
CD4:CD8 ratio comparison between cohorts of HIV-positive Asians and Caucasians upon commencement of antiretroviral therapy.Antivir Ther. 2017;22(8):659-668. doi: 10.3851/IMP3155. Antivir Ther. 2017. PMID: 28291735 Free PMC article.
-
Trends in mortality among ART-treated HIV-infected adults in the Asia-Pacific region between 1999 and 2017: results from the TREAT Asia HIV Observational Database (TAHOD) and Australian HIV Observational Database (AHOD) of IeDEA Asia-Pacific.J Int AIDS Soc. 2019 Jan;22(1):e25219. doi: 10.1002/jia2.25219. J Int AIDS Soc. 2019. PMID: 30615271 Free PMC article.
-
Trends in Follow-Up Visits Among People Living With HIV: Results From the TREAT Asia and Australian HIV Observational Databases.J Acquir Immune Defic Syndr. 2021 Sep 1;88(1):70-78. doi: 10.1097/QAI.0000000000002725. J Acquir Immune Defic Syndr. 2021. PMID: 33990493 Free PMC article.
-
Timing of initiation of antiretroviral therapy in AIDS-free HIV-1-infected patients: a collaborative analysis of 18 HIV cohort studies.Lancet. 2009 Apr 18;373(9672):1352-63. doi: 10.1016/S0140-6736(09)60612-7. Epub 2009 Apr 8. Lancet. 2009. PMID: 19361855 Free PMC article. Review.
-
From CD4-Based Initiation to Treating All HIV-Infected Adults Immediately: An Evidence-Based Meta-analysis.Front Immunol. 2018 Feb 13;9:212. doi: 10.3389/fimmu.2018.00212. eCollection 2018. Front Immunol. 2018. PMID: 29487595 Free PMC article.
Cited by
-
CD4:CD8 ratio comparison between cohorts of HIV-positive Asians and Caucasians upon commencement of antiretroviral therapy.Antivir Ther. 2017;22(8):659-668. doi: 10.3851/IMP3155. Antivir Ther. 2017. PMID: 28291735 Free PMC article.
-
Rates and factors associated with major modifications to first-line combination antiretroviral therapy: results from the Asia-Pacific region.PLoS One. 2013 Jun 28;8(6):e64902. doi: 10.1371/journal.pone.0064902. Print 2013. PLoS One. 2013. PMID: 23840312 Free PMC article.
-
Differences in lipid measurements by antiretroviral regimen exposure in cohorts from Asia and australia.AIDS Res Treat. 2012;2012:246280. doi: 10.1155/2012/246280. Epub 2012 May 14. AIDS Res Treat. 2012. PMID: 22675613 Free PMC article.
References
-
- World Health Organisation. HIV /AIDS in the South-East Asia Region. [Accessed June 15, 2010];2009 http://www.searo.who.int/LinkFiles/Publications_HIV_AIDS_Report2009.pdf.
-
- Hammer SM, Eron JJ, Jr, Reiss P, et al. Antiretroviral treatment of adult HIV infection: 2008 recommendations of the International AIDS Society-USA panel. JAMA. 2008;300(5):555–570. - PubMed
-
- Kadhiravan T, Sharma SK. Mortality of HIV-infected patients in low-income countries. Lancet. 2006;368(9554):2207–2207. - PubMed
-
- World Health Organisation. Rapid advice: Antiretroviral therapy for HIV infectionin adults and adolescents. [Accessed June 15, 2010];2009 http://www.who.int/hiv/pub/arv/rapid_advice_art.pdf.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials