

Prognosis of invasive intraductal papillary mucinous neoplasm depends on histological and precursor epithelial subtypes
- PMID: 21508421
- PMCID: PMC3806085
- DOI: 10.1136/gut.2010.232272
Prognosis of invasive intraductal papillary mucinous neoplasm depends on histological and precursor epithelial subtypes
Abstract
Objective: Invasive cancers arising from intraductal papillary mucinous neoplasm (IPMN) are recognised as a morphologically and biologically heterogeneous group of neoplasms. Less is known about the epithelial subtypes of the precursor IPMN from which these lesions arise. The authors investigate the clinicopathological characteristics and the impact on survival of both the invasive component and its background IPMN.
Design and patients: The study cohort comprised 61 patients with invasive IPMN (study group) and 570 patients with pancreatic ductal adenocarcinoma (PDAC, control group) resected at a single institution. Multivariate analyses were performed using a stage-matched Cox proportional hazard model.
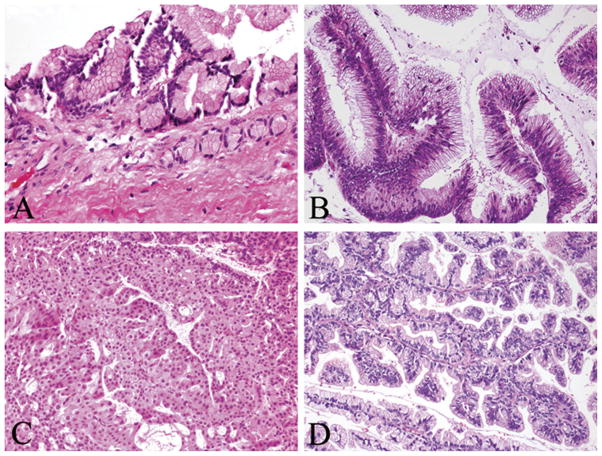
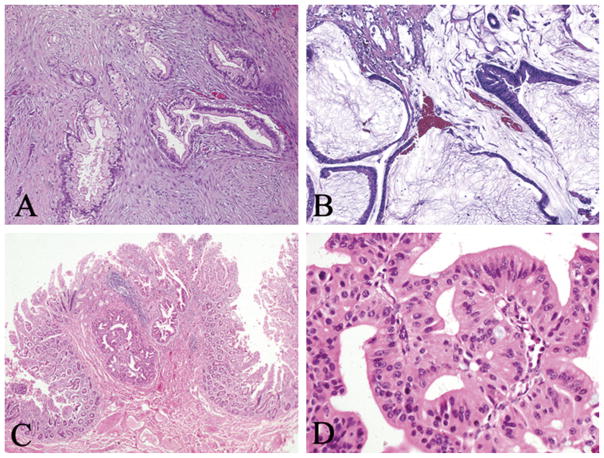
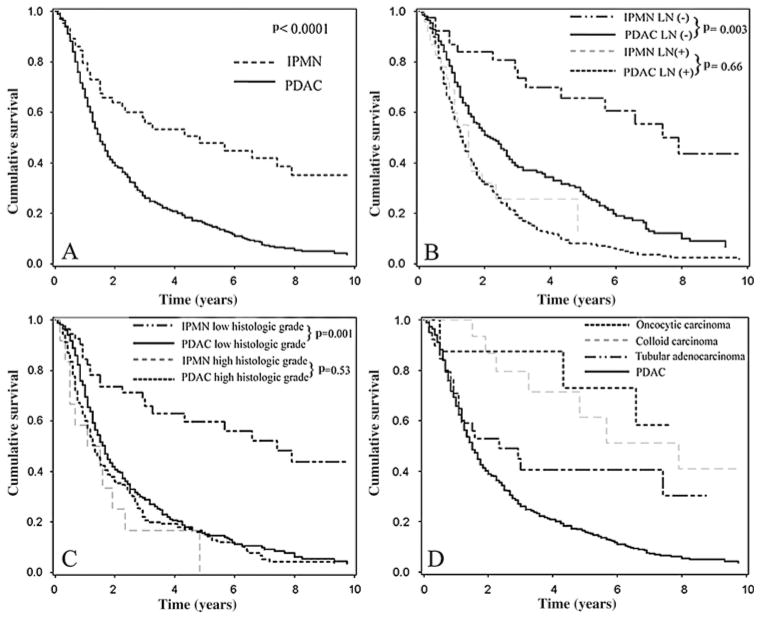
Results: The histology of invasive components of the IPMN cohort was tubular in 38 (62%), colloid in 16 (26%), and oncocytic in seven (12%). Compared with PDAC, invasive IPMNs were associated with a lower incidence of adverse pathological features and improved mortality by multivariate analysis (HR 0.58; 95% CI 0.39 to 0.86). In subtype analysis, this favourable outcome remained only for colloid and oncocytic carcinomas, while tubular adenocarcinoma was associated with worse overall survival, not significantly different from that of PDAC (HR 0.85; 95% CI 0.53 to 1.36). Colloid and oncocytic carcinomas arose only from intestinal- and oncocytic-type IPMNs, respectively, and were mostly of the main-duct type, whereas tubular adenocarcinomas primarily originated in the gastric background, which was often associated with branch-duct IPMN. Overall survival of patients with invasive adenocarcinomas arising from gastric-type IPMN was significantly worse than that of patients with non-gastric-type IPMN (p=0.016).
Conclusions: Tubular, colloid and oncocytic invasive IPMNs have varying prognosis, and arise from different epithelial subtypes. Colloid and oncocytic types have markedly improved biology, whereas the tubular type has a course that resembles PDAC. Analysis of these subtypes indicates that the background epithelium plays an equally, if not more, important role in defining the biology and prognosis of invasive IPMNs.
Conflict of interest statement
Figures
References
-
- Hruban RH, Pitman MB, Klimstra DS. Intraductal neoplasms. In: Hruban RH, Pitman MB, Klimstra DS, editors. Tumors of the Pancreas. Washington, DC: Amrican Registry of Pathology; 2007. pp. 75–110.
-
- Farrell JJ, Brugge WR. Intraductal papillary mucinous tumor of the pancreas. Gastrointest Endosc. 2002;55:701–14. - PubMed
-
- Longnecker DS, Adler G, Hruban RH, et al. Intraductal papillary-mucinous neoplasms of the pancreas. In: Hamilton SR, Aaltonen LA, editors. Pathology and Genetics of Tumors of the Digestive System. Lyon: IARC Press; 2000. pp. 237–40.
-
- Yamao K, Ohashi K, Nakamura T, et al. The prognosis of intraductal papillary mucinous tumors of the pancreas. Hepatogastroenterology. 2000;47:1129–34. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical