

Clinical development of experimental therapies for malignant glioma
- PMID: 21509204
- PMCID: PMC3074673
Clinical development of experimental therapies for malignant glioma
Abstract
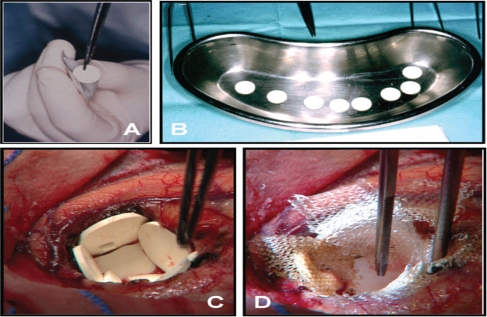
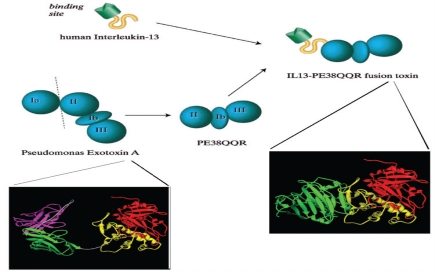
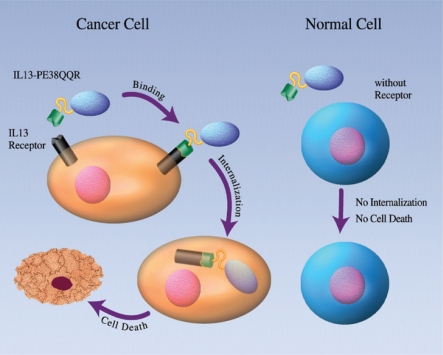
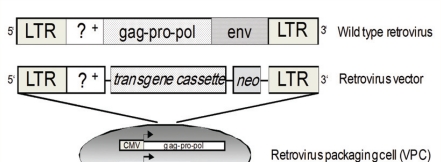
Advances in medical and surgical treatments in the last two to three decades have resulted in quantum leaps in the overall survival of patients with many types of non-central nervous system (CNS) malignant disease, while survival of patients with malignant gliomas (WHO grades 3 and 4) has only moderately improved. Surgical resection, external fractionated radiotherapy and oral chemotherapy, during and after irradiation, remain the pillars of malignant glioma therapy and have shown significant benefits. However, numerous clinical trials with adjuvant agents, most of them administered systemically and causing serious complications and side effects, have not achieved a noteworthy extension of survival, or only with considerable deterioration in patients' quality of life. Significant attention was focussed in the last decades on the cell biology and molecular genetics of gliomas. Improved understanding of the fundamental features of tumour cells has resulted in the introduction and increasing clinical use of local therapies, which employ spatially defined delivery methods and tumour-selective agents specifically designed to be used in the environment of a glioma-invaded brain. This review summarises the key findings of some of the most recent and important clinical studies of locally administered novel treatments for malignant glioma. Several such therapies have shown considerable anti-tumour activity and a favourable profile of local and systemic side effects. These include biodegradable polymers for interstitial chemotherapy, targeted toxins administered by convection enhanced delivery, and intra- and peritumourally injected genetically modified viruses conferring glioma-selective toxicity. Areas of possible improvement of these therapies and essential future developments are also outlined.
Keywords: Astrocytoma; Convection-enhanced delivery; Glioma; Immunotoxin; Virus.
Figures
Similar articles
-
Novel therapies for malignant gliomas: a local affair?Neurosurg Focus. 2006 Apr 15;20(4):E9. Neurosurg Focus. 2006. PMID: 16709040 Review.
-
Clinical development of experimental virus-mediated gene therapy for malignant glioma.Anticancer Agents Med Chem. 2011 Oct;11(8):739-47. doi: 10.2174/187152011797378724. Anticancer Agents Med Chem. 2011. PMID: 21707496 Review.
-
Current status of local therapy in malignant gliomas--a clinical review of three selected approaches.Pharmacol Ther. 2013 Sep;139(3):341-58. doi: 10.1016/j.pharmthera.2013.05.003. Epub 2013 May 18. Pharmacol Ther. 2013. PMID: 23694764 Review.
-
Present and potential future adjuvant issues in high-grade astrocytic glioma treatment.Adv Tech Stand Neurosurg. 2009;34:3-35. doi: 10.1007/978-3-211-78741-0_1. Adv Tech Stand Neurosurg. 2009. PMID: 19368079 Review.
-
Convection-enhanced delivery of targeted toxins for malignant glioma.Expert Opin Drug Deliv. 2006 May;3(3):371-7. doi: 10.1517/17425247.3.3.371. Expert Opin Drug Deliv. 2006. PMID: 16640497 Review.
Cited by
-
Expression of EphrinB2 and EphB4 in glioma tissues correlated to the progression of glioma and the prognosis of glioblastoma patients.Clin Transl Oncol. 2012 Mar;14(3):214-20. doi: 10.1007/s12094-012-0786-2. Clin Transl Oncol. 2012. PMID: 22374425
-
Expression of transforming growth factor-β1 (TGF-β1) and E-cadherin in glioma.Tumour Biol. 2012 Oct;33(5):1477-84. doi: 10.1007/s13277-012-0398-z. Epub 2012 Apr 29. Tumour Biol. 2012. PMID: 22544614
-
TNF receptor-associated factor 6 regulates proliferation, apoptosis, and invasion of glioma cells.Mol Cell Biochem. 2013 May;377(1-2):87-96. doi: 10.1007/s11010-013-1573-2. Epub 2013 Jan 29. Mol Cell Biochem. 2013. Retraction in: Mol Cell Biochem. 2016 Apr;415(1-2):207. doi: 10.1007/s11010-016-2682-5. PMID: 23358926 Retracted.
-
Overexpression of SASH1 related to the decreased invasion ability of human glioma U251 cells.Tumour Biol. 2012 Dec;33(6):2255-63. doi: 10.1007/s13277-012-0487-z. Epub 2012 Aug 23. Tumour Biol. 2012. PMID: 22915266
-
Gene therapy for malignant glioma.Mol Cell Ther. 2014 Jul 8;2:21. doi: 10.1186/2052-8426-2-21. eCollection 2014. Mol Cell Ther. 2014. PMID: 26056588 Free PMC article. Review.
References
-
- Kleihues P, Cavenee WK. Pathology and genetics of tumours of the nervous system. Lyon: IARC Press; 2000.
-
- Ohgaki H, Kleihues P. Population-based studies on incidence, survival rates, and genetic alterations in astrocytic and oligodendroglial gliomas. J Neuropathol Exp Neurol. 2005;64:479–89. - PubMed
-
- Davis FG, Freels S, Grutsch J, Barlas S, Brem S. Survival rates in patients with primary malignant brain tumors stratified by patient age and tumor histological type: an analysis based on surveillance, epidemiology, and end results (SEER) data, 1973–1991. J Neurosurg. 1998;88:1–10. - PubMed
-
- Davis FG, McCarthy BJ, Berger MS. Centralized databases available for describing primary brain tumor incidence, survival, and treatment: Central brain tumor registry of the United States; surveillance, epidemiology, and end results; and National cancer data base. Neurooncol. 1999;1:205–11. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases