

Practical advice for determining the role of BCR-ABL mutations in guiding tyrosine kinase inhibitor therapy in patients with chronic myeloid leukemia
- PMID: 21509757
- PMCID: PMC4180713
- DOI: 10.1002/cncr.25717
Practical advice for determining the role of BCR-ABL mutations in guiding tyrosine kinase inhibitor therapy in patients with chronic myeloid leukemia
Erratum in
- Cancer. 2011 Aug;117(15):3535
Abstract
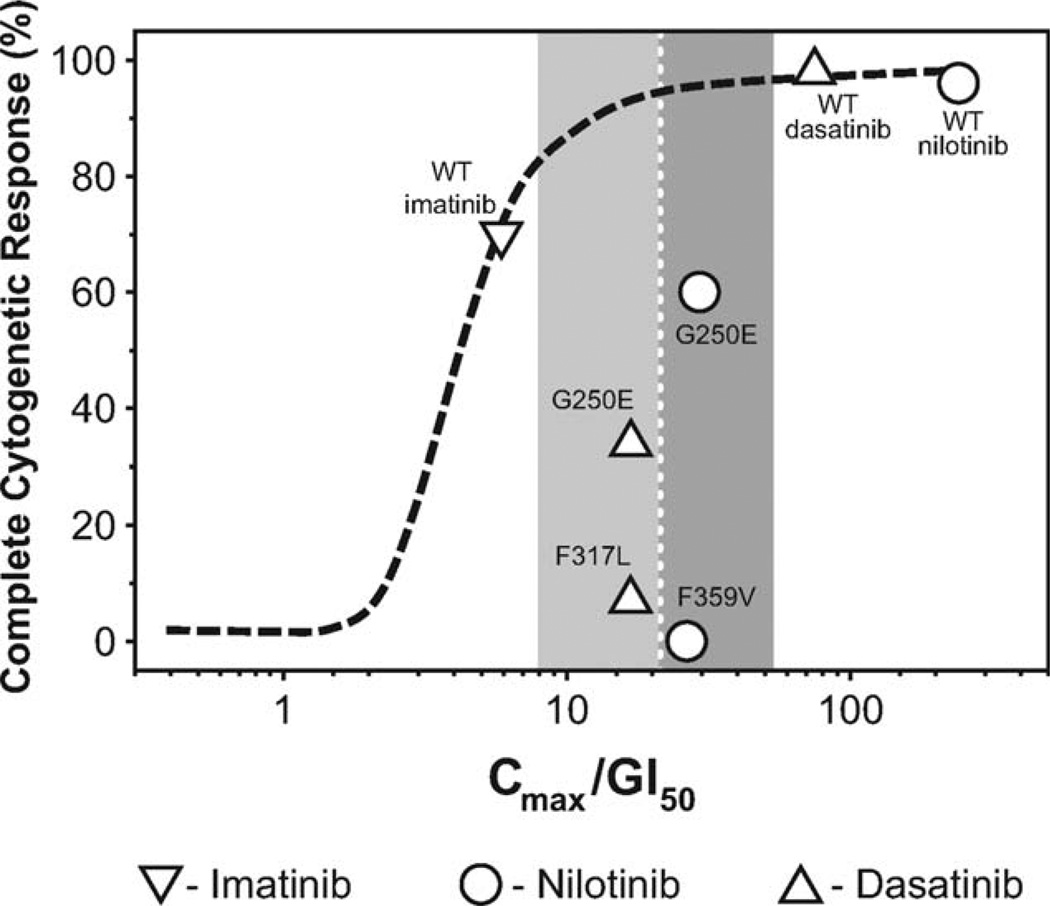
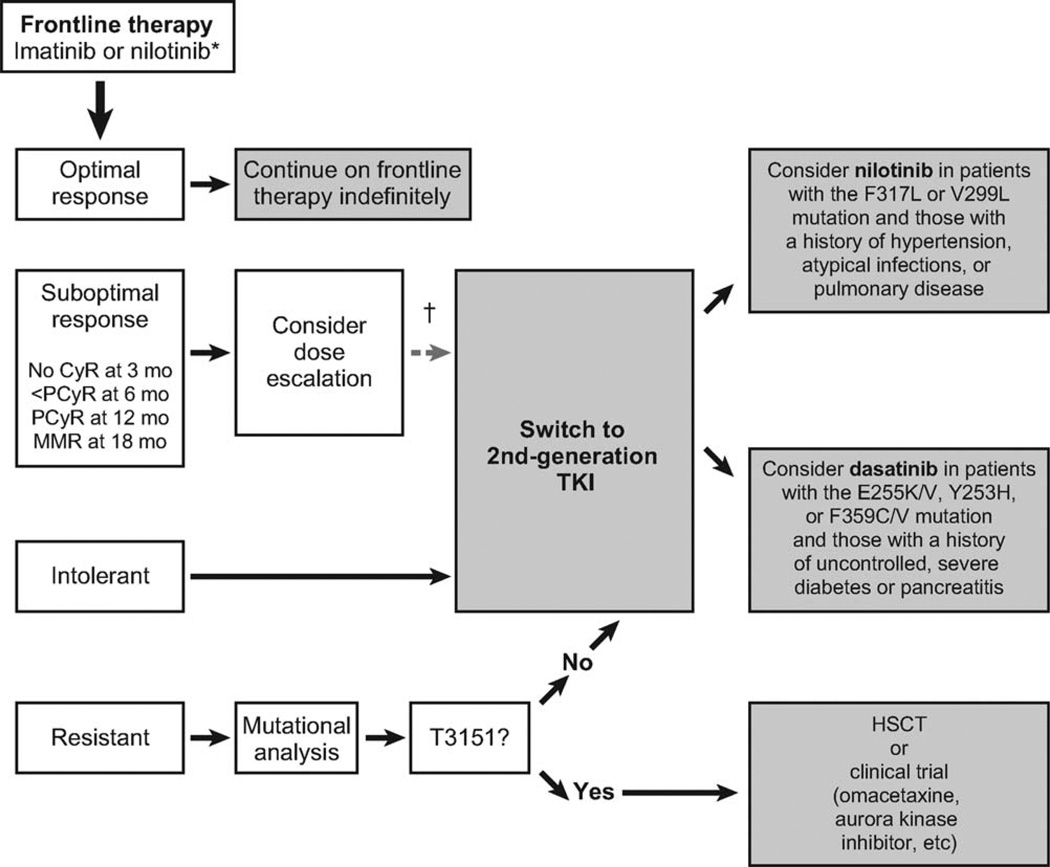
Data demonstrating the superiority of nilotinib over imatinib in the frontline treatment of chronic myeloid leukemia (CML) and ongoing studies with dasatinib and bosutinib are rapidly changing the treatment landscape for CML. In this review, the authors discuss currently available therapies for CML, focusing on mechanisms of resistance to imatinib and treatment strategies to overcome resistance. Relevant articles were identified through searches of PubMed and abstracts from international hematology/oncology congresses. Additional information sources were identified from the bibliographies of these references and from the authors' own libraries and expertise. In vitro 50% inhibitory concentration (IC(50) ) data alone are not sufficient to guide the choice of a tyrosine kinase inhibitor (TKI) in the presence of a mutant breakpoint cluster region-v-abl Abelson murine leukemia viral oncogene homolog (BCR-ABL) clone, because there is a lack of data regarding how well such IC(50) values correlate with clinical response. A small subset of BCR-ABL mutant clones have been associated with impaired responses to second-generation TKIs (tyrosine to histidine mutation at codon 253 [Y253H], glutamic acid to lysine or valine mutation at codon 255 [E255K/V], and phenylalanine to cysteine or valine mutation at codon 359 [F359C/V] for nilotinib; valine to leucine mutation at codon 299 [V299L] and F317L for dasatinib); neither nilotinib nor dasatinib is active against the threonine to isoleucine mutation at codon 315 (T315I). For each second-generation TKI, the detection of 1 of a small subset of mutations at the time of resistance may be helpful in the selection of second-line therapy [corrected]. For the majority of patients, comorbidities and drug safety profiles should be the basis for choosing a second-line agent. Clinical trial data from an evaluation of the response of specific mutant BCR-ABL clones to TKIs is needed to establish the role of mutation testing in the management of CML.
Copyright © 2010 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
Dr. Jones has no conflicts of interest to declare.
Figures
References
-
- O’Brien SG, Guilhot F, Larson RA, et al. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2003;348:994–1004. - PubMed
-
- Hochhaus A, O’Brien SG, Guilhot F, et al. Six-year follow-up of patients receiving imatinib for the first-line treatment of chronic myeloid leukemia. Leukemia. 2009;23:1054–1061. - PubMed
-
- National Comprehensive Cancer Network. Chronic Myelogenous Leukemia. Version 2. Jenkintown, PA: NCCN; 2010. NCCN: Clinical Practice Guidelines in Oncology. - PubMed
-
- Shah NP. Medical management of CML. Hematology Am Soc Hematol Educ Program. 2007:371–375. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
