

Laparoscopic extraperitoneal para-aortic lymphadenectomy in locally advanced cervical cancer: a prospective correlation of surgical findings with positron emission tomography/computed tomography findings
- PMID: 21509770
- PMCID: PMC4286384
- DOI: 10.1002/cncr.25739
Laparoscopic extraperitoneal para-aortic lymphadenectomy in locally advanced cervical cancer: a prospective correlation of surgical findings with positron emission tomography/computed tomography findings
Abstract
Background: Failure to detect metastasis to para-aortic nodes in patients with locally advanced cervical cancer leads to suboptimal treatment. No previous studies have prospectively compared positron emission tomography (PET)/computed tomography (CT) with laparoscopic extraperitoneal staging in the evaluation of para-aortic lymph nodes.
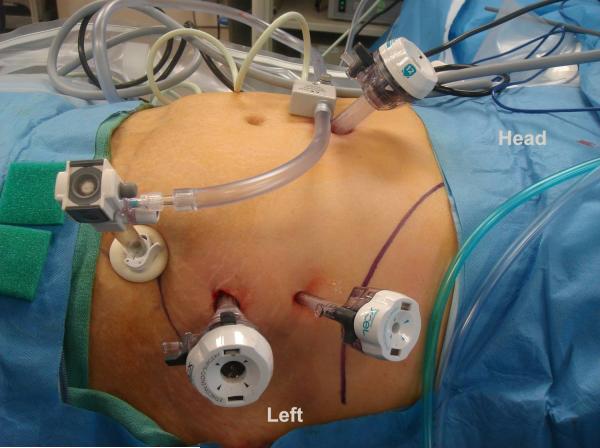
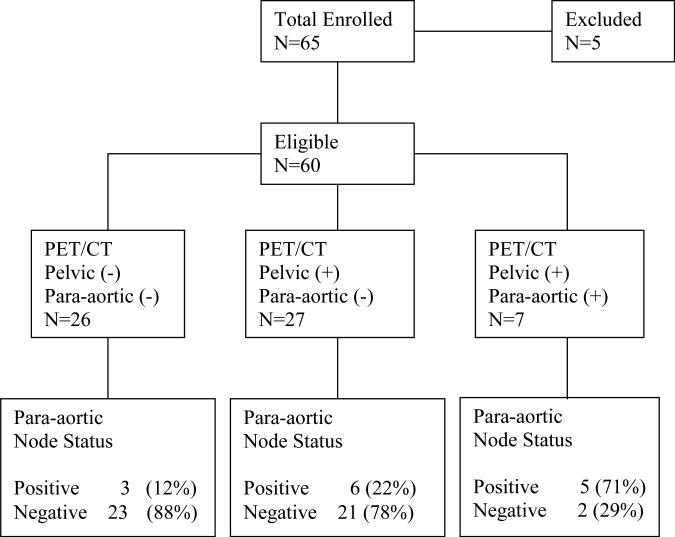
Methods: Sixty-five patients were enrolled; 60 were available for analysis. Patients with stage IB2-IVA cervical cancer without evidence of para-aortic lymphadenopathy on preoperative CT or magnetic resonance imaging (MRI) were prospectively enrolled. All patients underwent preoperative PET/CT. Laparoscopic extraperitoneal lymphadenectomy was performed from the common iliac vessels to the left renal vein.
Results: The median age at diagnosis was 48 years (range, 23-84). The median operative time was 140 minutes (range, 89-252). The median blood loss was 22.5 mL (range, 5-150). The median length of hospital stay was 1 day (range, 0-4). The median number of lymph nodes retrieved was 11 (range, 1-39). Fourteen (23%) patients had histopathologically positive para-aortic nodes. Of the 26 patients with negative pelvic and para-aortic nodes on PET/CT, 3 (12%) had histopathologically positive para-aortic nodes. Of the 27 patients with positive pelvic but negative para-aortic nodes on PET/CT, 6 (22%) had histopathologically positive para-aortic nodes. The sensitivity and specificity of PET/CT in detecting positive para-aortic nodes when nodes were negative on CT or MRI were 36% and 96%, respectively. Eleven (18.3%) patients had a treatment modification based on surgical findings.
Conclusions: Laparoscopic extraperitoneal para-aortic lymphadenectomy is safe and feasible. Surgical staging of patients with locally advanced cervical cancer should be considered before planned radiation and chemotherapy.
Copyright © 2010 American Cancer Society.
Figures
References
-
- Lagasse LD, Creasman WT, Shingleton HM, et al. Results and complications of operative staging in cervical cancer: Experience of the Gynecologic Oncology Group. Gynecol Oncol. 1980;9:90–98. - PubMed
-
- Stehman FB, Bundy BN, DiSaia PJ, et al. Carcinoma of the cervix treated with radiation therapy: A multi-variate analysis of prognostic variables in the Gynecologic Oncology Group. Cancer. 1991;67:2776–2785. - PubMed
-
- Berman ML, Lagasse LD, Watring WG, et al. The operative evaluation of patients with cervical carcinoma by an extraperitoneal approach. Obstet Gynecol. 1977;50:658–664. - PubMed
-
- Querleu D, Dargent D, Ansquer Y, et al. Extraperitoneal endosurgical aortic and common iliac dissection in the staging of bulky or advanced cervical carcinomas. Cancer. 2000;88:1883–1891. - PubMed
-
- Vergote I, Pouseele B, van Gorp T, et al. Robotic retroperitoneal lower para-aortic lymphadenectomy in cervical carcinoma: first report on the technique used in 5 patients. Acta Ostet Gynecol Scand. 2008;87:783–787. - PubMed
