

The outcome of neutrophil gelatinase-associated lipocalin-positive subclinical acute kidney injury: a multicenter pooled analysis of prospective studies
- PMID: 21511111
- PMCID: PMC4866647
- DOI: 10.1016/j.jacc.2010.11.051
The outcome of neutrophil gelatinase-associated lipocalin-positive subclinical acute kidney injury: a multicenter pooled analysis of prospective studies
Abstract
Objectives: The aim of this study was to test the hypothesis that, without diagnostic changes in serum creatinine, increased neutrophil gelatinase-associated lipocalin (NGAL) levels identify patients with subclinical acute kidney injury (AKI) and therefore worse prognosis.
Background: Neutrophil gelatinase-associated lipocalin detects subclinical AKI hours to days before increases in serum creatinine indicate manifest loss of renal function.
Methods: We analyzed pooled data from 2,322 critically ill patients with predominantly cardiorenal syndrome from 10 prospective observational studies of NGAL. We used the terms NGAL(-) or NGAL(+) according to study-specific NGAL cutoff for optimal AKI prediction and the terms sCREA(-) or sCREA(+) according to consensus diagnostic increases in serum creatinine defining AKI. A priori-defined outcomes included need for renal replacement therapy (primary endpoint), hospital mortality, their combination, and duration of stay in intensive care and in-hospital.
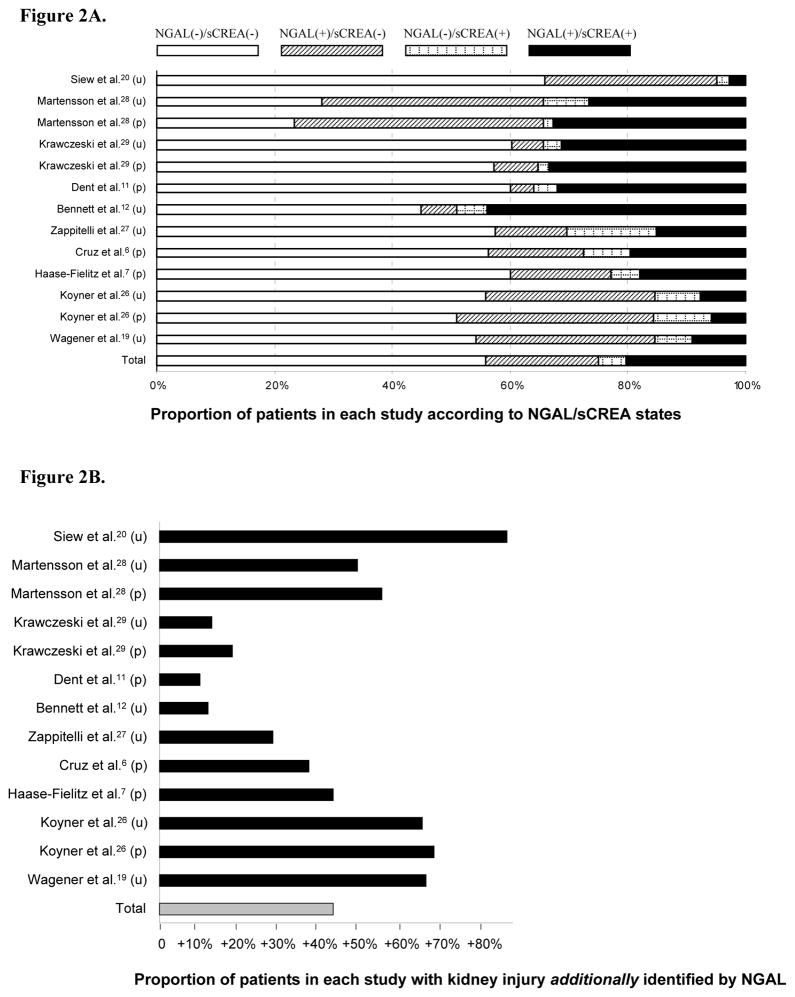
Results: Of study patients, 1,296 (55.8%) were NGAL(-)/sCREA(-), 445 (19.2%) were NGAL(+)/sCREA(-), 107 (4.6%) were NGAL(-)/sCREA(+), and 474 (20.4%) were NGAL(+)/sCREA(+). According to the 4 study groups, there was a stepwise increase in subsequent renal replacement therapy initiation-NGAL(-)/sCREA(-): 0.0015% versus NGAL(+)/sCREA(-): 2.5% (odds ratio: 16.4, 95% confidence interval: 3.6 to 76.9, p < 0.001), NGAL(-)/sCREA(+): 7.5%, and NGAL(+)/sCREA(+): 8.0%, respectively, hospital mortality (4.8%, 12.4%, 8.4%, 14.7%, respectively) and their combination (4-group comparisons: all p < 0.001). There was a similar and consistent progressive increase in median number of intensive care and in-hospital days with increasing biomarker positivity: NGAL(-)/sCREA(-): 4.2 and 8.8 days; NGAL(+)/sCREA(-): 7.1 and 17.0 days; NGAL(-)/sCREA(+): 6.5 and 17.8 days; NGAL(+)/sCREA(+): 9.0 and 21.9 days; 4-group comparisons: p = 0.003 and p = 0.040, respectively. Urine and plasma NGAL indicated a similar outcome pattern.
Conclusions: In the absence of diagnostic increases in serum creatinine, NGAL detects patients with likely subclinical AKI who have an increased risk of adverse outcomes. The concept and definition of AKI might need re-assessment.
Copyright © 2011 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures




Comment in
-
Early detection of acute kidney injury with neutrophil gelatinase-associated lipocalin.J Am Coll Cardiol. 2011 Apr 26;57(17):1762-4. doi: 10.1016/j.jacc.2010.11.050. J Am Coll Cardiol. 2011. PMID: 21511112 No abstract available.
References
-
- Uchino S, Bellomo R, Goldsmith D, et al. An assessment of the RIFLE criteria for acute renal failure in hospitalized patients. Crit Care Med. 2006;34:1913–7. - PubMed
-
- Haase M, Bellomo R, Matalanis G, et al. A comparison of the RIFLE and Acute Kidney Injury Network classifications for cardiac surgery-associated acute kidney injury: a prospective cohort study. J Thorac Cardiovasc Surg. 2009;138:1370–6. - PubMed
-
- Mishra J, Dent C, Tarabishi R, et al. Neutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renal injury after cardiac surgery. Lancet. 2005;365:1231–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
