

Pictorial review of mucopolysaccharidosis with emphasis on MRI features of brain and spine
- PMID: 21511751
- PMCID: PMC3473658
- DOI: 10.1259/bjr/59197814
Pictorial review of mucopolysaccharidosis with emphasis on MRI features of brain and spine
Abstract
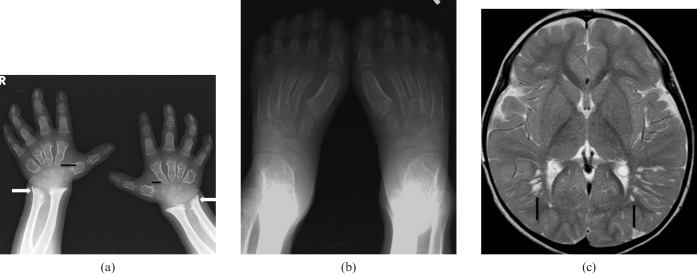
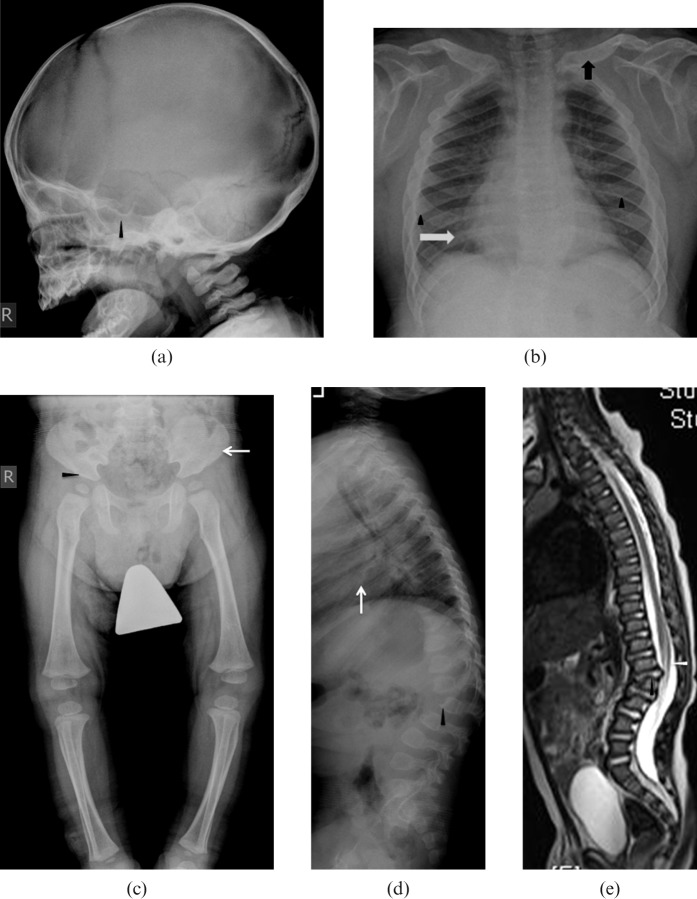
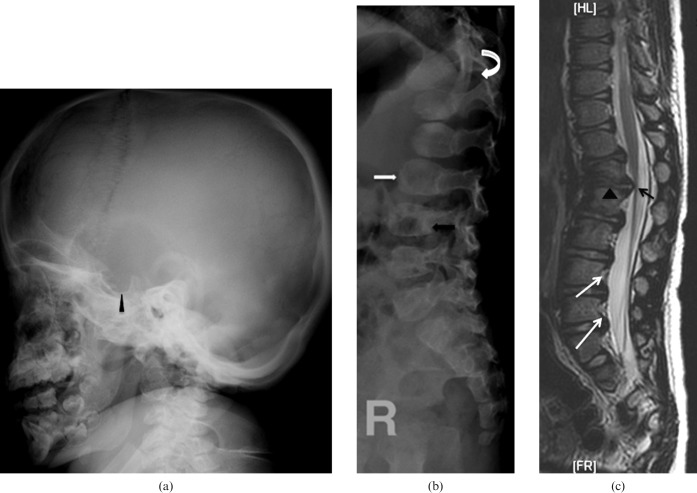
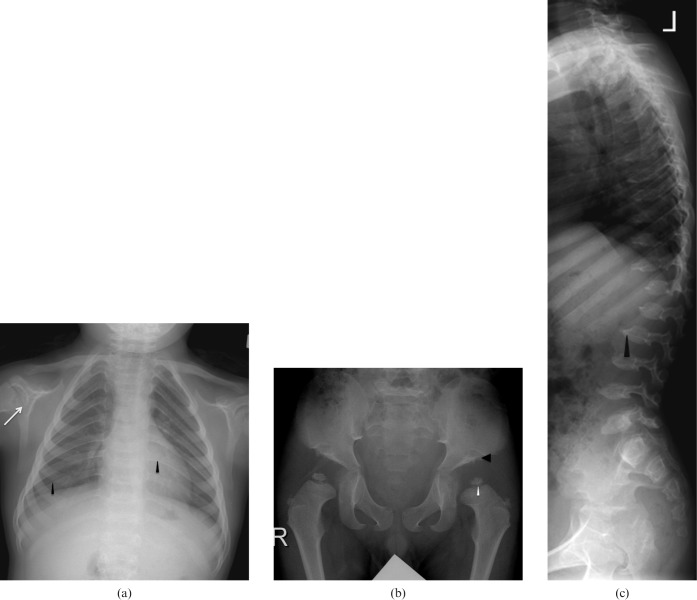
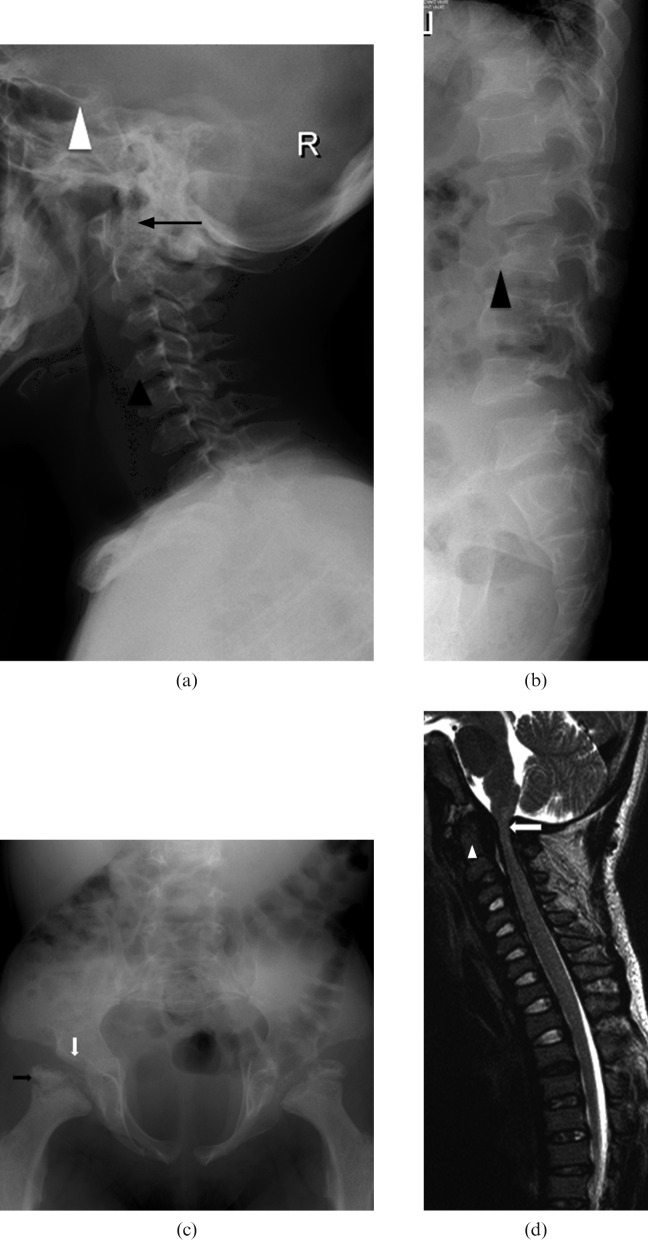
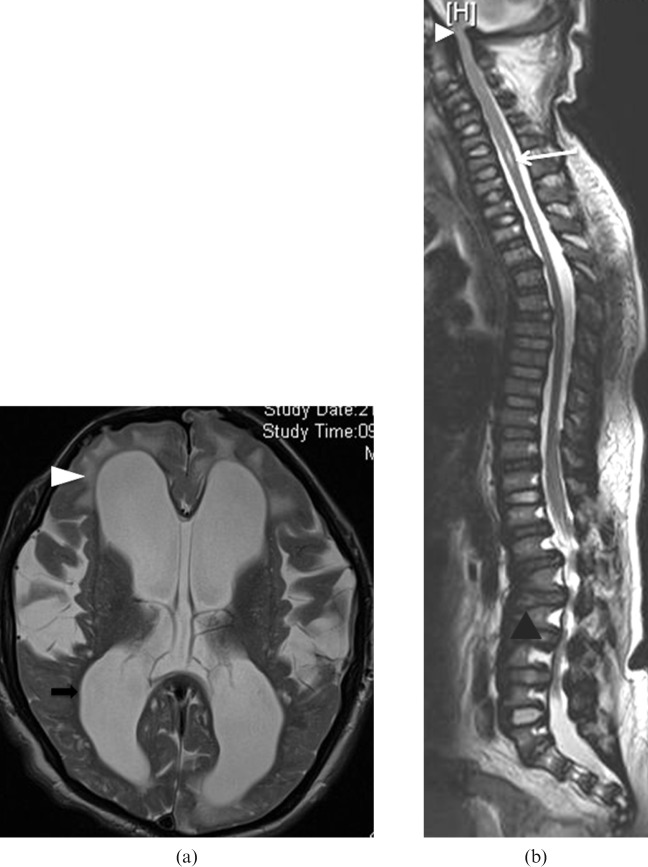
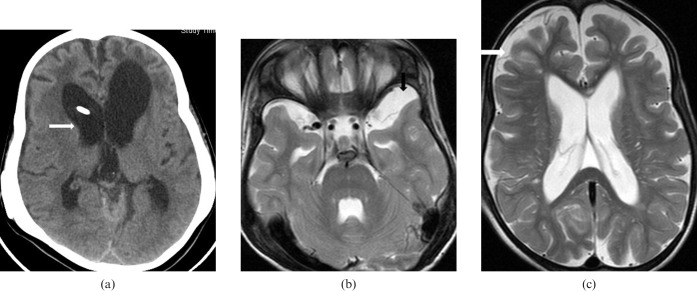
Mucopolysaccharidosis (MPS) is an inherited metabolic disorder of childhood, characterised by progressive multisystem involvement predominantly affecting the skeletal system leading to skeletal dysplasia. Mental retardation, neuropathy and cardiomyopathy may occur in the most severely affected patients, leading to progressive disability and death in their early third to fourth decades. The purpose of this paper is to illustrate the typical imaging features of different types of MPS, in particular the MR features of the brain and spine in MPS, which are expected to be encountered by radiologists more frequently in their clinical practice as a result of prolonged life expectancy for those with MPS with recent advances in therapeutic interventions. The treatment options and outcomes for MPS patients are also briefly discussed.
Figures
References
-
- Morquio L. Sur une forme de dystrophie osseuse familiale. Archives de médicine des infants 1929;32:129–35
-
- Goidanich IF, Lenzi L. Morquio- Ullrich Disease. A new mucopolysaccharidosis. J Bone Joint Surg Am 1964;46:734–46 - PubMed
-
- Langer LO., Jr Spondyloepiphysial dysplasia tarda. Hereditary chondrodysplasia with characteristic vertebral configuration in the adult. Radiology 1964;82:833–9 - PubMed
-
- Langer LO, Jr, Carey LS. The roentgenographic features of the KS mucopolysaccharidosis of Morquio (Morquio-Brailsford's disease). Am J Roentgenol Radium Ther Nucl Med 1966;97:1–20 - PubMed
-
- Kaendler S, Bockenheimer S, Grafin Vitzthum H, Galow W. Cervical myelopathy in mucopolysaccharidosis type II (Hunter's syndrome). Neuroradiologic, clinical and histopathologic findings. Dtsch Med Wochenschr 1990;115:1348–52 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
