

Pirfenidone for diabetic nephropathy
- PMID: 21511828
- PMCID: PMC3103734
- DOI: 10.1681/ASN.2010101049
Pirfenidone for diabetic nephropathy
Abstract
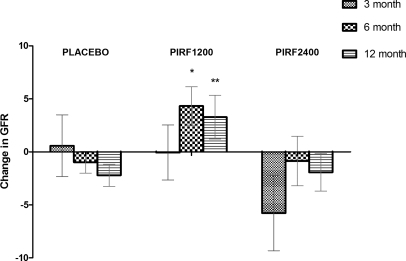
Pirfenidone is an oral antifibrotic agent that benefits diabetic nephropathy in animal models, but whether it is effective for human diabetic nephropathy is unknown. We conducted a randomized, double-blind, placebo-controlled study in 77 subjects with diabetic nephropathy who had elevated albuminuria and reduced estimated GFR (eGFR) (20 to 75 ml/min per 1.73 m²). The prespecified primary outcome was a change in eGFR after 1 year of therapy. We randomly assigned 26 subjects to placebo, 26 to pirfenidone at 1200 mg/d, and 25 to pirfenidone at 2400 mg/d. Among the 52 subjects who completed the study, the mean eGFR increased in the pirfenidone 1200-mg/d group (+3.3 ± 8.5 ml/min per 1.73 m²) whereas the mean eGFR decreased in the placebo group (-2.2 ± 4.8 ml/min per 1.73 m²; P = 0.026 versus pirfenidone at 1200 mg/d). The dropout rate was high (11 of 25) in the pirfenidone 2400-mg/d group, and the change in eGFR was not significantly different from placebo (-1.9 ± 6.7 ml/min per 1.73 m²). Of the 77 subjects, 4 initiated hemodialysis in the placebo group, 1 in the pirfenidone 2400-mg/d group, and none in the pirfenidone 1200-mg/d group during the study (P = 0.25). Baseline levels of plasma biomarkers of inflammation and fibrosis significantly correlated with baseline eGFR but did not predict response to therapy. In conclusion, these results suggest that pirfenidone is a promising agent for individuals with overt diabetic nephropathy.
Figures
Comment in
-
Trials and tribulations of new agents, novel biomarkers, and retarding renal progression.J Am Soc Nephrol. 2011 Jun;22(6):992-3. doi: 10.1681/ASN.2011040402. Epub 2011 May 26. J Am Soc Nephrol. 2011. PMID: 21617124 No abstract available.
References
-
- Steffes MW, Osterby R, Chavers B, Mauer SM: Mesangial expansion as a central mechanism for loss of kidney function in diabetic patients. Diabetes 38: 1077–1081, 1989 - PubMed
-
- Lane PH, Steffes M, Fioretto P, Mauer S: Renal interstitial expansion in insulin-dependent diabetes mellitus. Kidney Int 43: 661–667, 1993 - PubMed
-
- Fioretto P, Steffes M, Sutherland D, Mauer M: Sequential renal biopsies in insulin-dependent diabetic patients: Structural factors associated with clinical progression. Kidney Int 48: 1929–1935, 1995 - PubMed
-
- Lewis E, Hunsicker L, Bain R, Rohde R: The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. N Engl J Med 329: 1456–1462, 1993 - PubMed
-
- Brenner B, Cooper M, Zeeuw D, Keane W, Mitch W, Parving H-H, Remuzzi G, Snapinn S, Zhang Z, Shahinfar S: Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 345: 861–869, 2001 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
