

MR imaging findings in patients with secondary intracranial hypertension
- PMID: 21511864
- PMCID: PMC8013120
- DOI: 10.3174/ajnr.A2463
MR imaging findings in patients with secondary intracranial hypertension
Abstract
Background and purpose: IH can alter the configuration of anatomic structures of the central nervous system. We determined the sensitivity and specificity of MR imaging to detect these changes in patients with secondary IH.
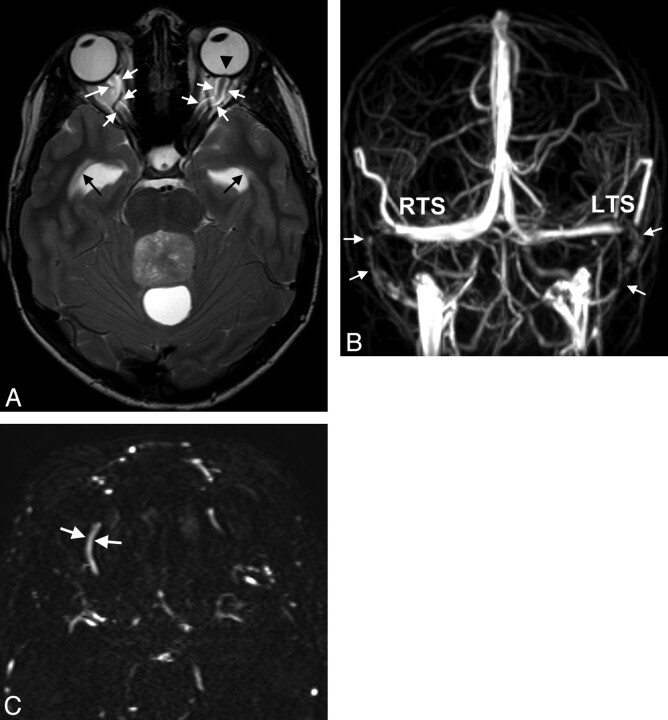
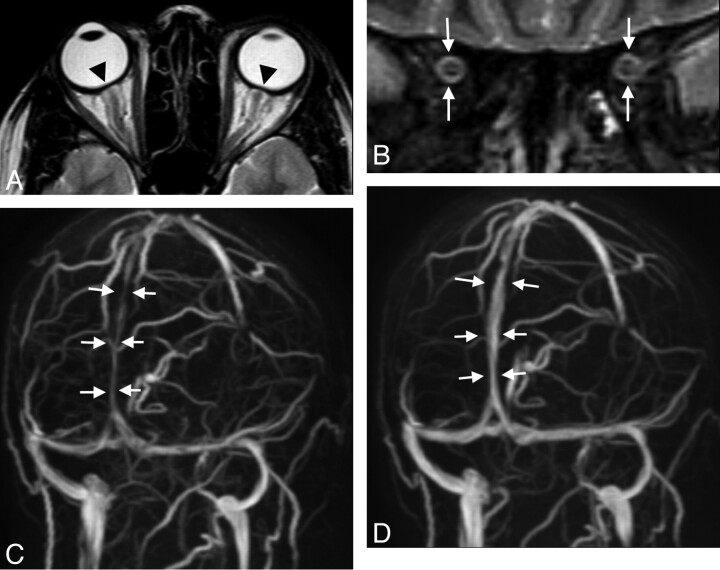
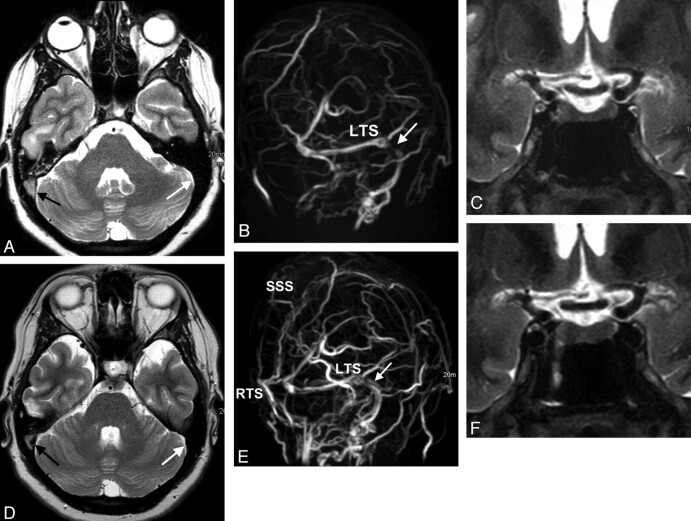
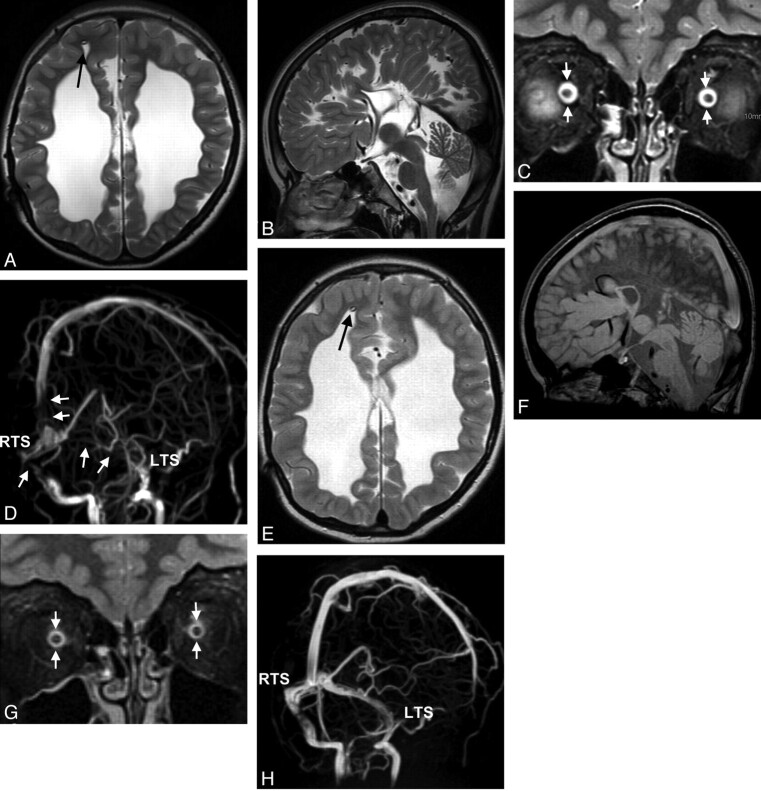
Materials and methods: Patients (n = 36) with IH were prospectively investigated with MR imaging and were matched to 36 controls. MR images were evaluated for elongation and edema of the optic nerves, protrusion of the optic disc, flattening of the posterior sclera, height of the pituitary gland, and width of the optic nerve sheath. On MRV, we recorded venous sinus abnormalities and measured the luminal width of the superior ophthalmic veins. A grading score was introduced to define cranial venous outflow obstruction.
Results: Cranial venous outflow obstruction and ONS hydrops were the most valid signs indicating IH with a sensitivity of 94% and 92% and a specificity of 100% and 89%, respectively. Sensitivities and specificities were 56% and 97% for reduced pituitary height, 64% and 78% for flattening of the posterior sclera, 31% and 97% for widening of the superior ophthalmic veins, 33% and 100% for optic disc protrusion, 14% and 100% for optic nerve edema, and 6% and 100% for elongation of the optic nerve. At least 2 MR imaging findings could be demonstrated in each patient but in none of the controls. The number of positive MR imaging findings correlated with CSF pressure (r = 0.62, P = .01).
Conclusions: The combination of cranial and orbital MR imaging and MRV can be highly sensitive and specific in the diagnosis of patients with IH.
Figures
References
-
- Ball AK, Clarke CE. Idiopathic intracranial hypertension. Lancet Neurol 2006; 5: 433– 42 - PubMed
-
- Binder DK, Horton JC, Lawton MT, et al. . Idiopathic intracranial hypertension. Neurosurgery 2004; 54: 538– 51, discussion 551–32 - PubMed
-
- Skau M, Brennum J, Gjerris F, et al. . What is new about idiopathic intracranial hypertension? An updated review of mechanism and treatment. Cephalalgia 2006; 26: 384– 99 - PubMed
-
- Bershad EM, Humphreis WE, Suarez JI. Intracranial hypertension. Semin Neurol 2008; 28: 690– 702 - PubMed
-
- Algahtani HA, Baeesa SS, Obeid TH, et al. . Idiopathic intracranial hypertension: atypical presentation. Saudi Med J 2007; 28: 762– 65 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical