

Bronchial secretory immunoglobulin a deficiency correlates with airway inflammation and progression of chronic obstructive pulmonary disease
- PMID: 21512171
- PMCID: PMC3265275
- DOI: 10.1164/rccm.201010-1629OC
Bronchial secretory immunoglobulin a deficiency correlates with airway inflammation and progression of chronic obstructive pulmonary disease
Abstract
Rationale: Although airway inflammation can persist for years after smoking cessation in patients with chronic obstructive pulmonary disease (COPD), the mechanisms of persistent inflammation are largely unknown.
Objectives: We investigated relationships between bronchial epithelial remodeling, polymeric immunoglobulin receptor (pIgR) expression, secretory IgA (SIgA), airway inflammation, and mural remodeling in COPD.
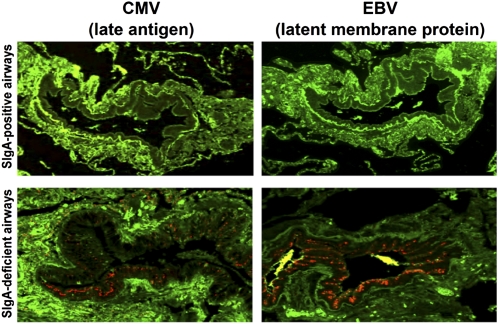
Methods: Lung tissue specimens and bronchoalveolar lavage were obtained from lifetime nonsmokers and former smokers with or without COPD. Epithelial structural changes were quantified by morphometric analysis. Expression of pIgR was determined by immunostaining and real-time polymerase chain reaction. Immunohistochemistry was performed for IgA, CD4 and CD8 lymphocytes, and cytomegalovirus and Epstein-Barr virus antigens. Total IgA and SIgA were measured by ELISA and IgA transcytosis was studied using cultured human bronchial epithelial cells.
Measurements and main results: Areas of bronchial mucosa covered by normal pseudostratified ciliated epithelium were characterized by pIgR expression with SIgA present on the mucosal surface. In contrast, areas of bronchial epithelial remodeling had reduced pIgR expression, localized SIgA deficiency, and increased CD4(+) and CD8(+) lymphocyte infiltration. In small airways (<2 mm), these changes were associated with presence of herpesvirus antigens, airway wall remodeling, and airflow limitation in patients with COPD. Patients with COPD had reduced SIgA in bronchoalveolar lavage. Air-liquid interface epithelial cell cultures revealed that complete epithelial differentiation was required for normal pIgR expression and IgA transcytosis.
Conclusions: Our findings indicate that epithelial structural abnormalities lead to localized SIgA deficiency in COPD airways. Impaired mucosal immunity may contribute to persistent airway inflammation and progressive airway remodeling in COPD.
Figures






Comment in
-
Secretory IgA and COPD: a new kid on the block?Am J Respir Crit Care Med. 2011 Aug 1;184(3):285-7. doi: 10.1164/rccm.201105-0821ED. Am J Respir Crit Care Med. 2011. PMID: 21804117 No abstract available.
-
From disease heterogeneity through patient endotype to "microtype": the future for chronic obstructive pulmonary disease research?Am J Respir Crit Care Med. 2012 Mar 15;185(6):686-7. doi: 10.1164/ajrccm.185.6.686a. Am J Respir Crit Care Med. 2012. PMID: 22422908 No abstract available.
References
-
- Rutgers SR, Postma DS, ten Hacken NH, Kauffman HF, Der Mark TW, Koeter GH, Timens W. Ongoing airway inflammation in patients with COPD who do not currently smoke. Thorax 2000;55:12–18 - PubMed
-
- Verra F, Escudier E, Lebargy F, Bernaudin JF, De CH, Bignon J. Ciliary abnormalities in bronchial epithelium of smokers, ex-smokers, and nonsmokers. Am J Respir Crit Care Med 1995;151:630–634 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
