

Efficacy and harms of nasal calcitonin in improving bone density in young patients with inflammatory bowel disease: a randomized, placebo-controlled, double-blind trial
- PMID: 21519359
- PMCID: PMC3150350
- DOI: 10.1038/ajg.2011.129
Efficacy and harms of nasal calcitonin in improving bone density in young patients with inflammatory bowel disease: a randomized, placebo-controlled, double-blind trial
Abstract
Objectives: There are very few published studies of agents having the potential to improve bone health in children with inflammatory bowel disease (IBD). The objective of this study was to establish the efficacy and safety of intranasal calcitonin in improving bone mineral density (BMD) in young patients with IBD and to define additional factors that impact bone mineral accrual.
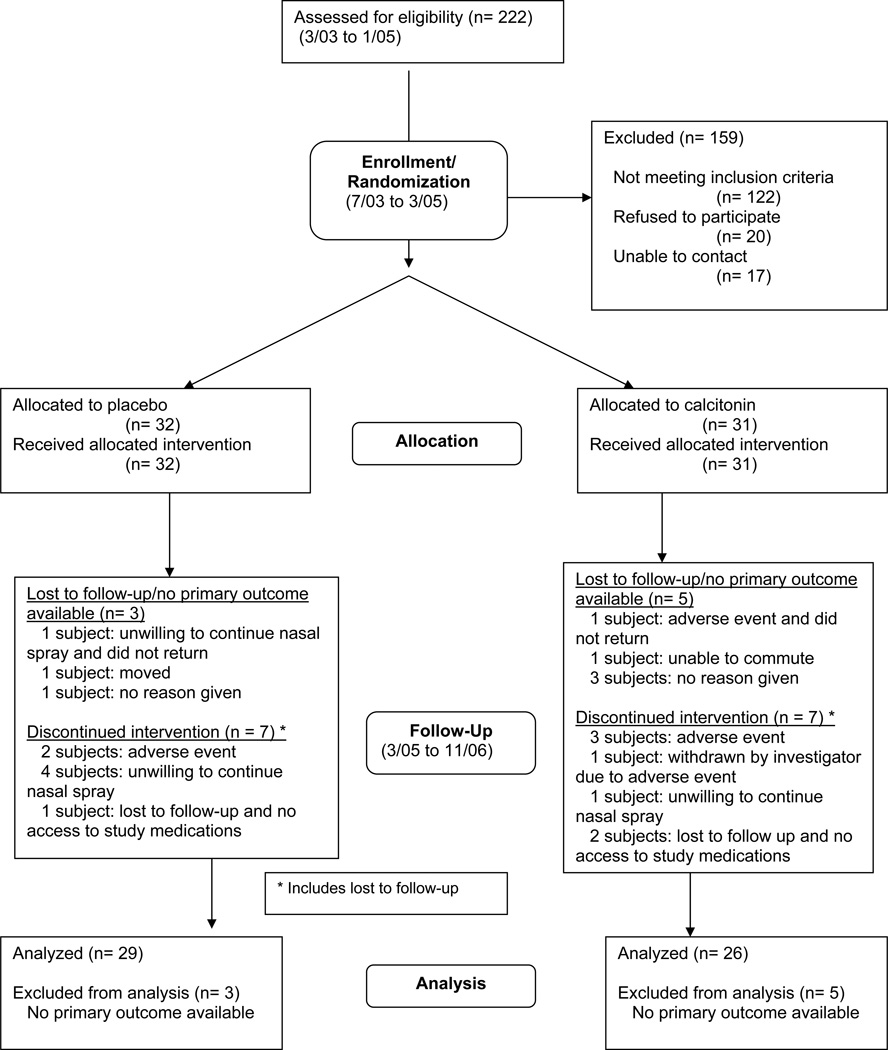
Methods: We conducted a randomized, placebo-controlled, double-blind clinical trial in 63 participants, ages 8-21 years, with a spinal BMD Z-score ≤ -1.0 s.d. measured by dual energy X-ray absorptiometry. Subjects were randomized to 200 IU intranasal calcitonin (n=31) or placebo (n=32) daily. All received age-appropriate calcium and vitamin D supplementation. Subsequent BMD measurements were obtained at 9 and 18 months.
Results: Intranasal calcitonin was well tolerated. Adverse event frequency was similar in both treatment groups, and such events were primarily minor, reversible, and limited to the upper respiratory tract. The BMD Z-score change documented at screening and 9 months and screening and 18 months did not differ between the two therapeutic arms. In participants with Crohn's disease, the spinal BMD Z-score improved between screening and 9 months (change in spine BMD Z-score (ΔZSBMD)(9-0)) in the calcitonin group (ΔZSBMD(9-0)(calcitonin)=0.21 (0.37), ΔZSBMD(9-0)(placebo)=-0.15 (0.5), P=0.02); however, this was only a secondary subgroup analysis. Bone mineral accrual rate during the trial did not lead to normalization of BMD Z-score in this cohort. Factors favoring higher bone mineral accrual rate were lower baseline BMD and higher baseline body mass index Z-score, improvement in height Z-score, higher serum albumin, hematocrit and iron concentration, and more hours of weekly weight-bearing activity. Factors associated with lower bone mineral accrual rate were more severe disease-as indicated by elevated inflammatory markers, need for surgery, hospitalization, and the use of immunomodulators-and higher daily caffeine intake.
Conclusions: Intranasal calcitonin is well tolerated but does not offer a long-term advantage in youth with IBD and decreased BMD. Bone mineral accrual rate remains compromised in youth with IBD and low BMD raising concerns for long-term bone health outcomes. Improvement in nutritional status, catch-up linear growth, control of inflammation, increase in weight-bearing activity, and lower daily caffeine intake may be helpful in restoring bone density in children with IBD and low BMD.
Conflict of interest statement
Dr Helen Pappa: No conflicts of interest exist
Tracee Saslowsky: No conflicts of interest exist
Rajna Filip-Dhima: No conflicts of interest exist
Dr Hajar Hassani Lahsinoui: No conflicts of interest exist
Apurva Akkad: No conflicts of interest exist
Dr Richard Grand: No conflicts of interest exist
Dr Catherine Gordon: Consultant: Gilead Sciences, Inc. and Director: Clinical Investigator Training Program, Harvard/MIT (with Pfizer/Merck)
Figures
References
-
- Gokhale R, Favus MJ, Karrison T, et al. Bone mineral density assessment in children with inflammatory bowel disease. Gastroenterology. 1998;114(5):902–911. - PubMed
-
- Sylvester FA, Wyzga N, Hyams JS, et al. Natural history of bone metabolism and bone mineral density in children with inflammatory bowel disease. Inflamm Bowel Dis. 2007;13(1):42–50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
