

Delirium in older emergency department patients is an independent predictor of hospital length of stay
- PMID: 21521405
- PMCID: PMC3768130
- DOI: 10.1111/j.1553-2712.2011.01065.x
Delirium in older emergency department patients is an independent predictor of hospital length of stay
Abstract
Objectives: The consequences of delirium in the emergency department (ED) remain unclear. This study sought to determine if delirium in the ED was an independent predictor of prolonged hospital length of stay (LOS).
Methods: This prospective cohort study was conducted at a tertiary care, academic ED from May 2007 to August 2008. The study included English-speaking patients aged 65 and older who were in the ED for less than 12 hours at enrollment. Patients were excluded if they refused consent, were previously enrolled, were unable to follow simple commands at baseline, were comatose, or did not have a delirium assessment performed by the research staff. The Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) was used to determine delirium status. Patients who were discharged directly from the ED were considered to have a hospital LOS of 0 days. To determine if delirium in the ED was independently associated with time to discharge, Cox proportional hazard regression was performed adjusted for age, comorbidity burden, severity of illness, dementia, functional impairment, nursing home residence, and surgical procedure. A sensitivity analysis, which included admitted patients only, was also performed.
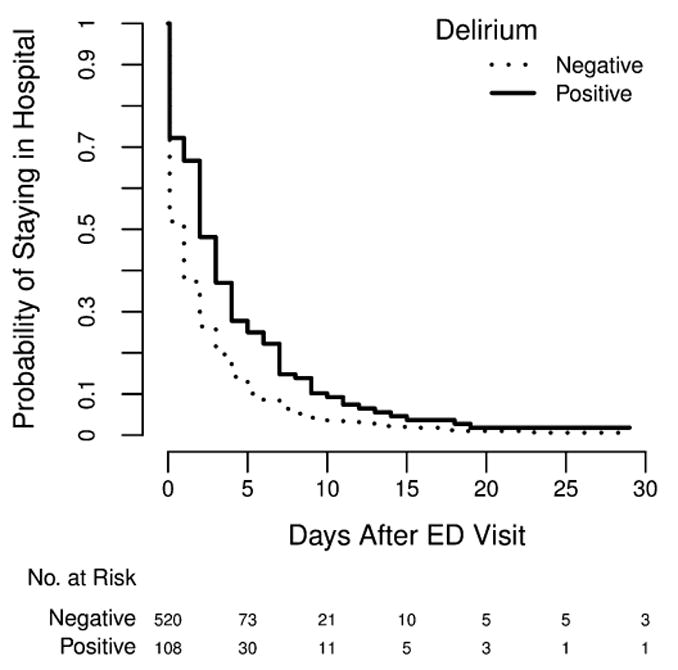
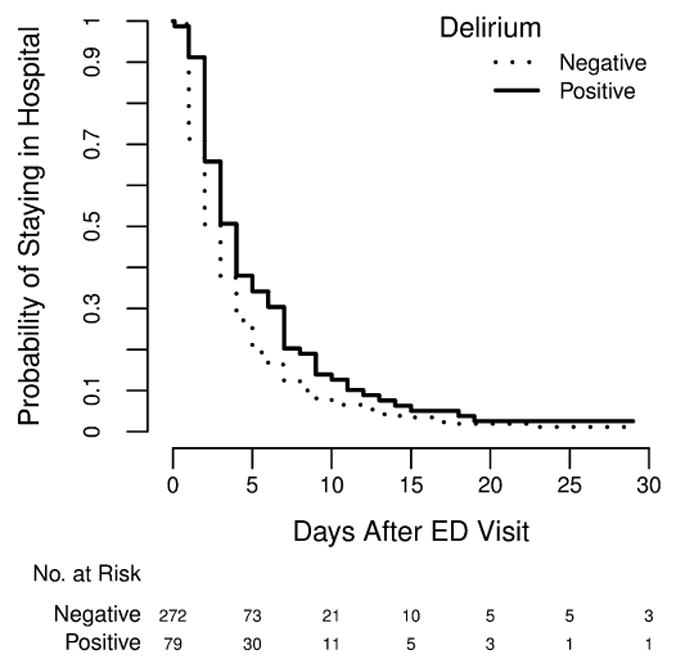
Results: A total of 628 patients met enrollment criteria. The median age was 75 years (interquartile range [IQR] = 69-81), 365 (58%) patients were female, 111 (18%) were nonwhite, 351 (56%) were admitted to the hospital, and 108 (17%) were delirious in the ED. Median LOS was 2 days (IQR = 0-5.5) for delirious ED patients and 1 day (IQR = 0-3) for nondelirious ED patients (p < 0.001). The hazard ratio (HR) of delirium for time to discharge was 0.71 (95% confidence interval [CI] = 0.57 to 0.89) after adjusting for confounders, and indicated that ED patients with delirium were more likely to have prolonged hospital LOS compared with those without delirium. For the sensitivity analysis, which included only hospitalized patients, the adjusted HR was 0.76 (95% CI = 0.58 to 0.99).
Conclusions: Delirium in older ED patients has negative consequences and is an independent predictor of prolonged hospitalizations.
© 2011 by the Society for Academic Emergency Medicine.
Figures
References
-
- Lewis LM, Miller DK, Morley JE, Nork MJ, Lasater LC. Unrecognized delirium in ED geriatric patients. Am J Emerg Med. 1995;13:142–5. - PubMed
-
- Hustey FM, Meldon SW, Smith MD, Lex CK. The effect of mental status screening on the care of elderly emergency department patients. Ann Emerg Med. 2003;41:678–84. - PubMed
-
- Francis J, Martin D, Kapoor WN. A prospective study of delirium in hospitalized elderly. JAMA. 1990;263:1097–101. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
