

Measurement of lung airways in three dimensions using hyperpolarized helium-3 MRI
- PMID: 21521907
- PMCID: PMC3159390
- DOI: 10.1088/0031-9155/56/10/014
Measurement of lung airways in three dimensions using hyperpolarized helium-3 MRI
Abstract
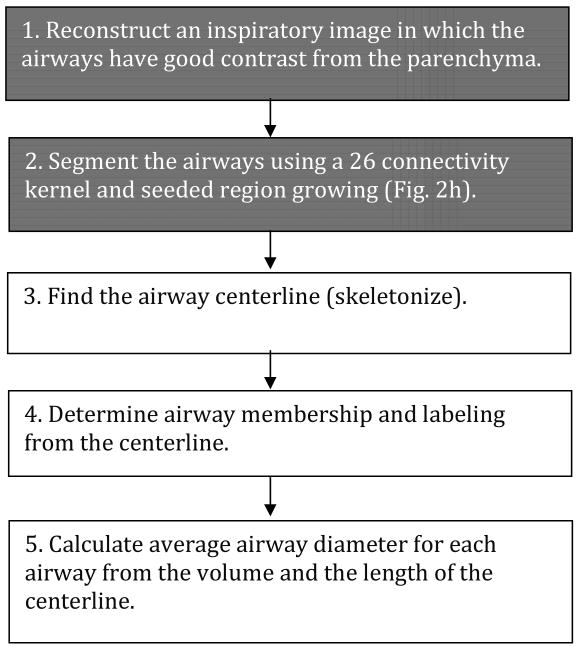
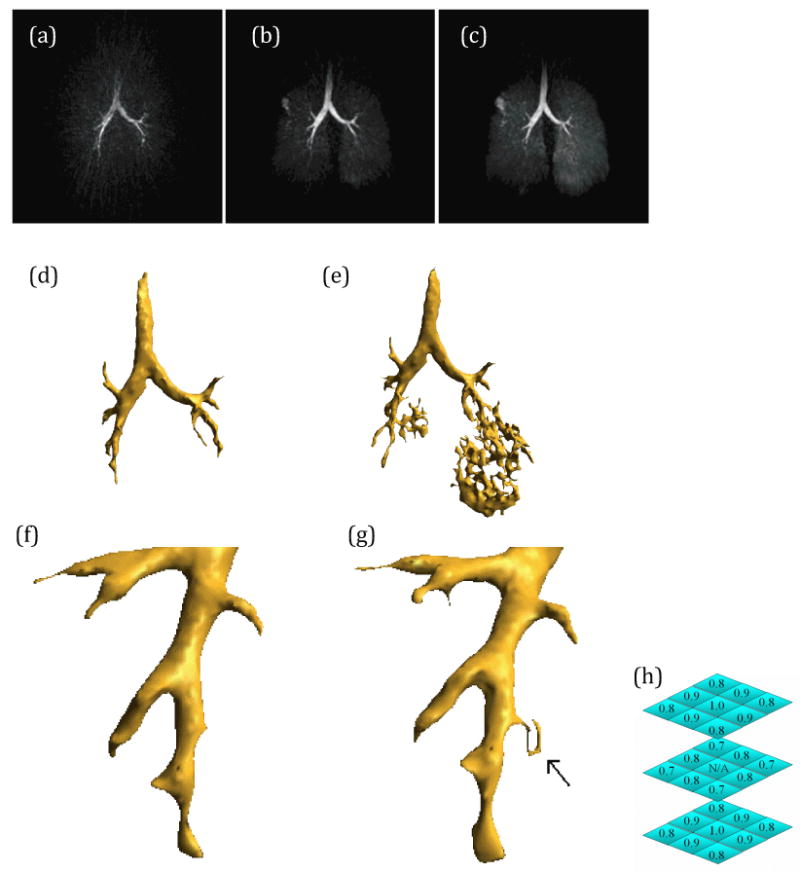
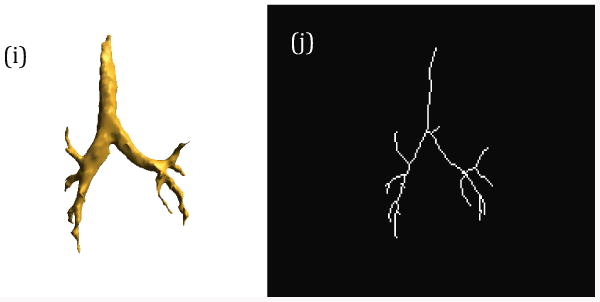
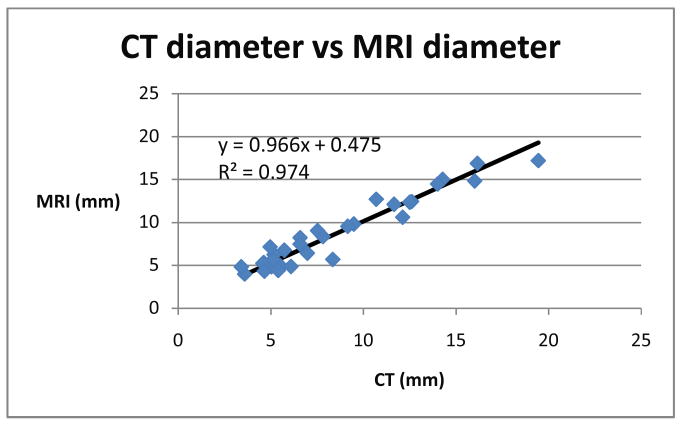
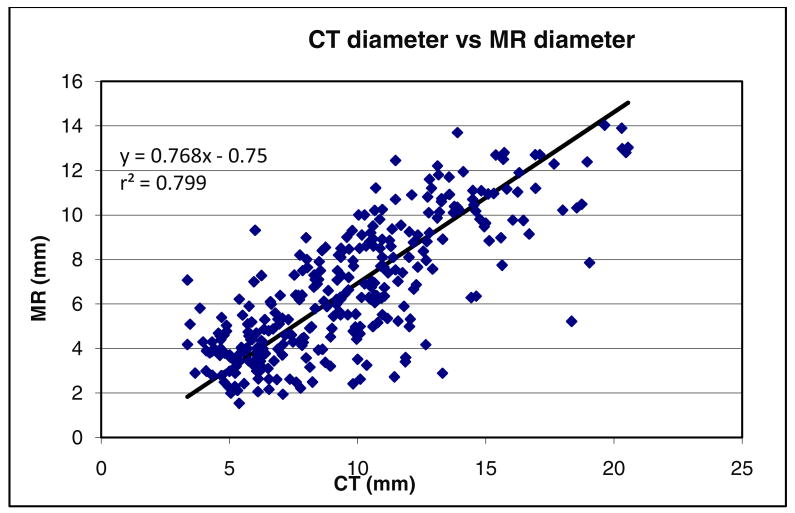
Large airway measurement is clinically important in cases of airway disease and trauma. The gold standard is computed tomography (CT), which allows for airway measurement. However, the ionizing radiation dose associated with CT is a major limitation in longitudinal studies and trauma. To avoid ionizing radiation from CT, we present a method for measuring the large airway diameter in humans using hyperpolarized helium-3 (HPHe) MRI in conjunction with a dynamic 3D radial acquisition. An algorithm is introduced which utilizes the significant airway contrast for semi-automated segmentation and skeletonization which is used to derive the airway lumen diameter. The HPHe MRI method was validated with quantitative CT in an excised and desiccated porcine lung (linear regression R(2) = 0.974 and slope = 0.966 over 32 airway segments). The airway lumen diameters were then compared in 24 human subjects (22 asthmatics and 2 normals; linear regression R(2) value of 0.799 and slope = 0.768 over 309 airway segments). The feasibility for airway path analysis to areas of ventilation defect is also demonstrated.
Figures
References
-
- Albert MS, Cates GD, Driehuys B, Happer W, Saam B, Springer CS, Jr, Wishnia A. Nature. Vol. 370. 1994. Biological magnetic resonance imaging using laser-polarized 129Xe; pp. 199–201. - PubMed
-
- Aysola RS, Hoffman EA, Gierada D, Wenzel S, Cook-Granroth J, Tarsi J, Zheng J, Schechtman KB, Ramkumar TP, Cochran R, Xueping E, Christie C, Newell J, Fain S, Altes TA, Castro M. Airway remodeling measured by multidetector CT is increased in severe asthma and correlates with pathology. Chest. 2008;134:1183–91. - PMC - PubMed
-
- Barger AV, Block WF, Toropov Y, Grist TM, Mistretta CA. Time-resolved contrast-enhanced imaging with isotropic resolution and broad coverage using an undersampled 3D projection trajectory. Magn Reson Med. 2002;48:297–305. - PubMed
-
- Brown RH, Mitzner W. Effect of lung inflation and airway muscle tone on airway diameter in vivo. J Appl Physiol. 1996;80:1581–8. - PubMed
-
- Brown RH, Mitzner W, Wagner E, Permutt S, Togias A. Airway distension with lung inflation measured by HRCT. Acad Radiol. 2003;10:1097–103. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical