

Non-operative rehabilitation for traumatic and atraumatic glenohumeral instability
- PMID: 21522197
- PMCID: PMC2953282
Non-operative rehabilitation for traumatic and atraumatic glenohumeral instability
Abstract
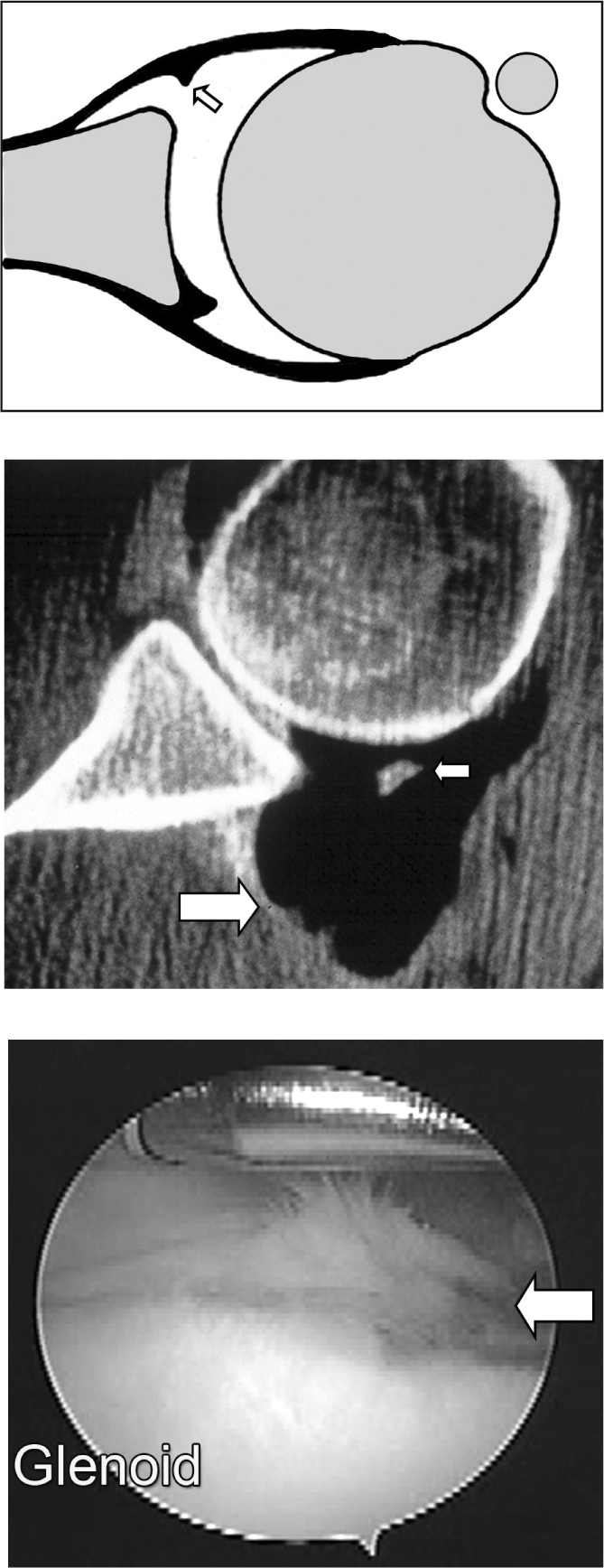
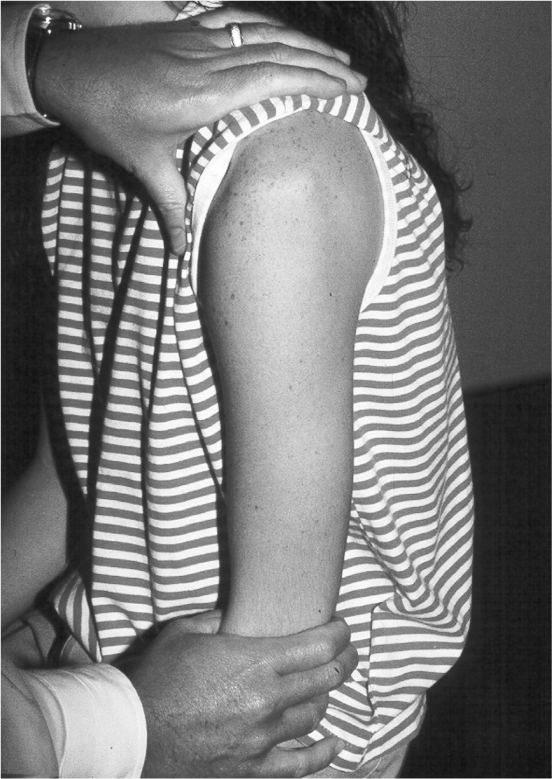
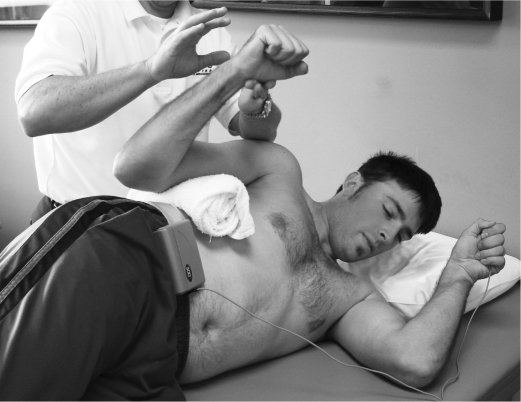
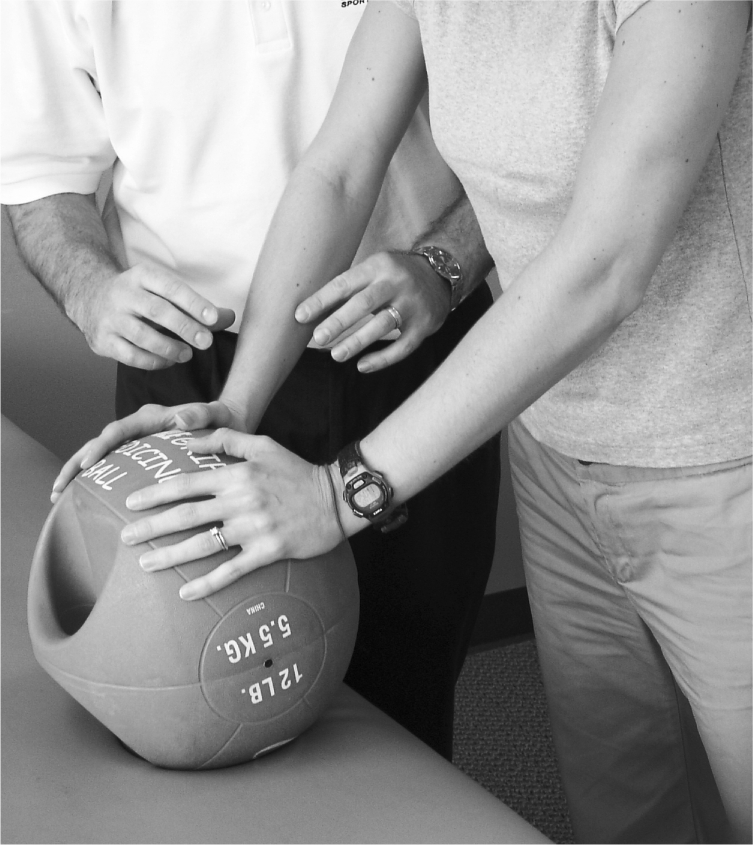
Glenohumeral joint instability is a common pathology encountered in the orthopaedic and sports medicine setting. A wide range of symptomatic shoulder instabilities exist ranging from subtle subluxations due to contributing congenital factors to dislocations as a result of a traumatic episode. Non-operative rehabilitation is utilized in patients diagnosed with shoulder instability to regain their previous functional activities through specific strengthening exercises, dynamic stabilization drills, neuromuscular training, proprioception drills, scapular muscle strengthening program and a gradual return to their desired activities. The specific rehabilitation program should be varied based on the type and degree of shoulder instability present and desired level of function. The purpose of this paper is to outline the specific principles associated with non-operative rehabilitation for each of the various types of shoulder instability and to discuss the specific rehabilitation program for each pathology type.
Figures








References
-
- Kibler WB. The role of the scapular in athletic shoulder function. Am J Sports Med. 1998;26:325–337 - PubMed
-
- Wilk KE, Arrigo CA, Andrews JR. Current concepts: The stabilizing structures of the glenohumeral joint. J Orthop Sports Phys Ther. 1997;25:364–379 - PubMed
-
- Speer KP, Deng X, Borrero S, et al. Biomechanical evaluation of a simulated Bankart lesion. J Bone Joint Surg. 1994;76A:1819–1826 - PubMed
-
- Warren RF, Kornblatt IB, Marchand R. Static factors affecting posterior shoulder instability. Orthop Trans. 1984;89
-
- Aronen JG, Regan K. Decreasing the incidence of recurrence of first time anterior dislocations with rehabilitation. Am J Sports Med. 1984;12:283–291 - PubMed
LinkOut - more resources
Full Text Sources