

De novo spine surgery as a predictor of additional spine surgery at the same or distant spine regions
- PMID: 21522488
- PMCID: PMC3080664
- DOI: 10.3205/000133
De novo spine surgery as a predictor of additional spine surgery at the same or distant spine regions
Abstract
Introduction: Degenerative spine disorders are steadily increasing parallel to the aging of the population with considerable impact on cost and productivity. In this paper we study the prevalence and risk factors for multiple spine surgery and its impact on cost.
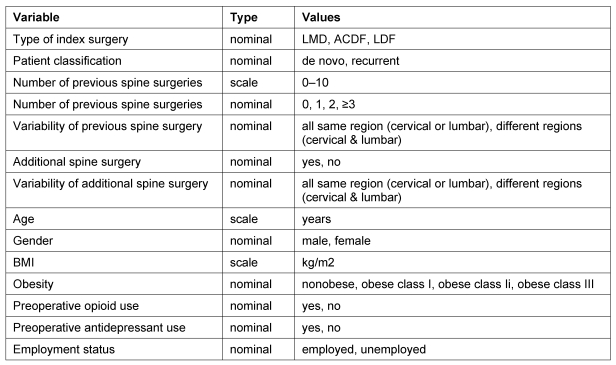
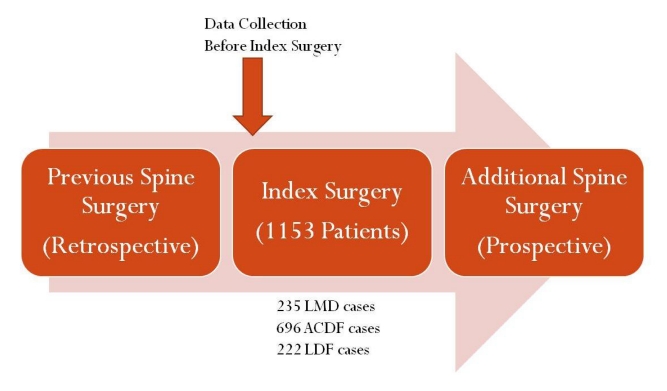
Methods: Data on 1,153 spine surgery inpatients operated between October 2005 and September 2008 (index spine surgery) in regard to the number of previous spine surgeries and location of surgeries (cervical or lumbar) were retrospectively collected. Additionally, prospective follow-up over a period of 2-5 years was conducted.
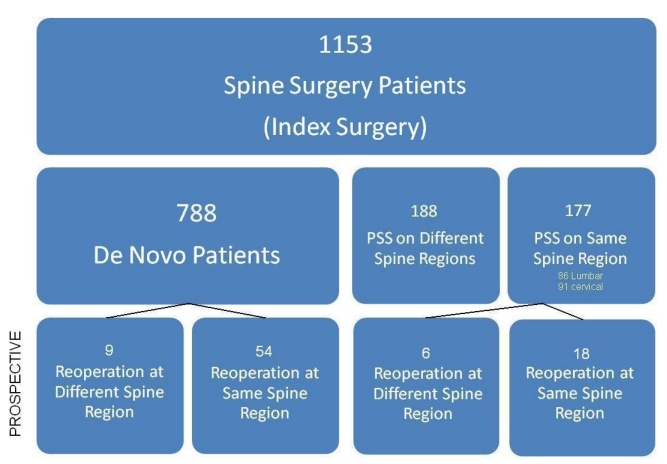
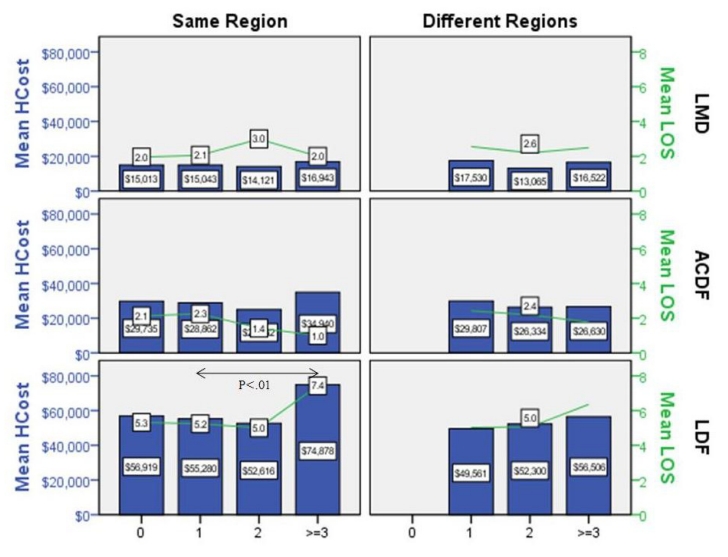
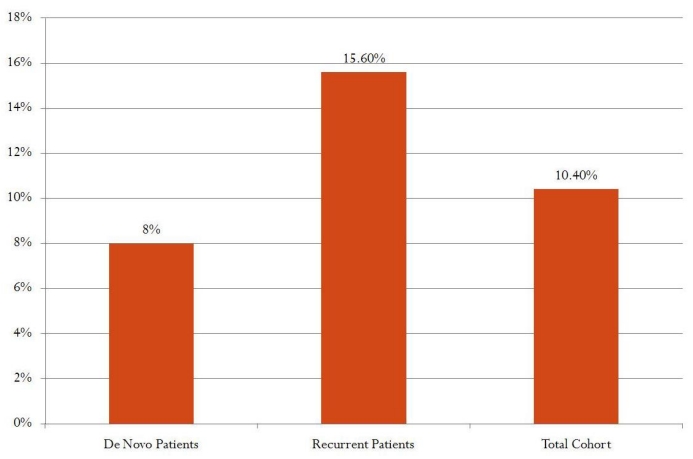
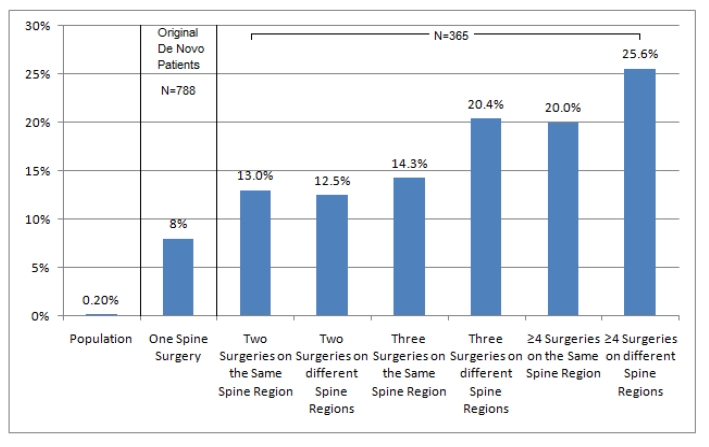
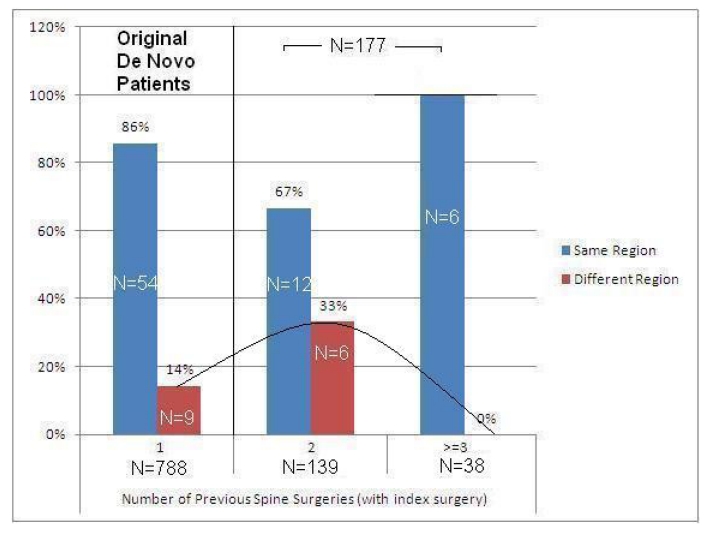
Results: Retrospectively, 365 (31.7%) patients were recurrent spine surgery patients while 788 (68.3%) were de novo spine surgery patients.Nearly half of those with previous spine surgery (51.5%) were on different regions of the spine. There were no significant differences in length of stay or hospital charges except in lumbar decompression and fusion (LDF) patients with multiple interventions on the same region of the spine. Significant differences (P<.05) in length of stay (5.4 days vs. 7.4 days) and hospital charges ($55,477 vs. $74,878) between LDF patients with one previous spine versus those with ≥3 previous spine surgeries on the same region were noted.Prospectively, the overall reoperation rate was 10.4%. The risk of additional spine surgery increased from 8.0% in patients with one previous spine surgery (index surgery) to 25.6% in patients with ≥4 previous spine surgeries on different regions of the spine (including index surgery).After excluding patients with previous spine surgeries on different regions of the spine, 17.2% of reoperated patients had additional spine surgery on a different spine region. The percentage of additional spine surgery on a distant spine region increased from 14.0% in patients with one spine surgery to 33.0% in patients with two spine surgeries on the same region. However, in patients with three or more spine surgeries on the same spine region there were no interventions on a distant spine region during the follow-up period.
Conclusion: De novo spine surgery is associated with an increased incidence of additional spine surgery at the same or distant spine regions. Large prospective studies with extended follow-up periods and multifaceted cost-outcome analysis are needed to refine the appropriateness of spine surgery.
Einführung: Wirbelsäulenerkrankungen nehmen parallel zur Alterung der Bevölkerung ständig zu mit beachtlichen Auswirkungen auf Kosten und Produktivität. In diesem Artikel werden die Prävalenz und die Risikofaktoren für mehrfache Wirbelsäulenoperationen und ihr Einfluss auf die Folgekosten untersucht.
Methoden: Eine retrospektive Analyse von 1.153 Krankenhauspatienten nach Wirbelsäulenoperationen im Zeitraum von Oktober 2005 bis September 2008 auch in Bezug auf vorausgegangene Wirbelsäulenoperationen und deren Lokalisation (Hals- oder Lendenwirbelsäule) wurde erstellt. Zusätzlich wurden die Nachuntersuchungen über 2–5 Folgejahre erfasst.
Ergebnisse: Rückblickend hatten 365 (31,7%) der Patienten wiederholte chirurgische Eingriffe an der Wirbelsäule, während bei 788 (68,3%) Patienten der operative Eingriff erstmalig erfolgte. Etwa bei der Hälfte (51,5%) der Patienten mit wiederholten Wirbelsäulenoperationen wurden diese in verschiedenen Bereichen durchgeführt.
Es gab keine signifikanten Unterschiede bei der Dauer des Klinikaufenthaltes oder bei den Klinikkosten außer bei Patienten mit lumbaler Dekompression und Fusion (LDF) mit mehrfachen Eingriffen im gleichen Operationsbereich. Signifikante Unterschiede (P<0,05) wurden gefunden beim Dauer des Klinikaufenthalts (5,5 Tage versus 7,4 Tage) und bei den Krankenhauskosten (55.477 $ versus 77.877 $) zwischen LDF-Patienten mit einer vorherigen Wirbelsäulenoperation verglichen mit Patienten mit drei und mehr vorausgegangenen Operationen in demselben Wirbelsäulenbereich.
Prospektiv lag die Häufigkeit erneuter Operationen durchschnittlich bei 10,4%. Das Risiko einer zusätzlichen Wirbelsäulenoperation stieg von 8,0% bei Patienten mit einer vorausgegangenen Wirbelsäulenoperation (Indexoperation) auf 25,6% bei Patienten mit 4 und mehr chirurgischen Eingriffen an verschiedenen Regionen der Wirbelsäule (incl. Indexoperation).
Nach Ausschluss aller Patienten mit vorausgegangenen Wirbelsäulenoperationen in verschiedenen Wirbelsäulenbereichen hatten 17,2% der erneut operierten Patienten eine zusätzliche Operation in einem anderen Wirbelsäulenbereich. Der Prozentsatz der zusätzlichen chirurgischen Eingriffe in einem entfernten Wirbelsäulenbereich lag bei Patienten mit einer Wirbelsäulenoperation bei 14% und stieg auf 33% bei Patienten mit zwei Operationen im selben Bereich. Jedoch gab es bei Patienten mit drei und mehr chirurgischen Eingriffen in der gleichen Wirbelsäulenregion während der Beobachtungsperiode keine weiteren Operationen in einer anderen Region.
Schlussfolgerung: Eine Erstoperation an der Wirbelsäule ist assoziiert mit einer erhöhten Häufigkeit von weiteren Wirbelsäulenoperationen im gleichen oder einem anderen Wirbelsäulenbereich. Große prospektive Studien mit längeren Beobachtungsperioden und Kosten-Nutzen-Analysen sind erforderlich, um die Angemessenheit von Wirbelsäulenoperationen in geeigneter Form bewerten zu können.
Keywords: cost; multiple spine surgery; spine region.
Figures
Similar articles
-
Recurrent spine surgery patients in hospital administrative database.Ger Med Sci. 2012;10:Doc03. doi: 10.3205/000154. Epub 2012 Feb 1. Ger Med Sci. 2012. PMID: 22355279 Free PMC article.
-
Outcomes and complications of diabetes mellitus on patients undergoing degenerative lumbar spine surgery.Spine (Phila Pa 1976). 2014 Sep 1;39(19):1596-604. doi: 10.1097/BRS.0000000000000482. Spine (Phila Pa 1976). 2014. PMID: 24983935 Free PMC article.
-
Factors predicting hospital stay, operative time, blood loss, and transfusion in patients undergoing revision posterior lumbar spine decompression, fusion, and segmental instrumentation.Spine (Phila Pa 1976). 2002 Apr 15;27(8):818-24. doi: 10.1097/00007632-200204150-00008. Spine (Phila Pa 1976). 2002. PMID: 11935103
-
Reoperation of decompression alone or decompression plus fusion surgeries for degenerative lumbar diseases: a systematic review.Eur Spine J. 2019 Jun;28(6):1371-1385. doi: 10.1007/s00586-018-5681-2. Epub 2018 Jun 28. Eur Spine J. 2019. PMID: 29956000
-
Systematic Review of Cost-Effectiveness Analyses in U.S. Spine Surgery.World Neurosurg. 2020 Oct;142:e32-e57. doi: 10.1016/j.wneu.2020.05.123. Epub 2020 May 21. World Neurosurg. 2020. PMID: 32446983
Cited by
-
Recurrent spine surgery patients in hospital administrative database.Ger Med Sci. 2012;10:Doc03. doi: 10.3205/000154. Epub 2012 Feb 1. Ger Med Sci. 2012. PMID: 22355279 Free PMC article.
-
Perioperative mortality after lumbar spinal fusion surgery: an analysis of epidemiology and risk factors.Eur Spine J. 2012 Aug;21(8):1633-9. doi: 10.1007/s00586-012-2298-8. Epub 2012 Apr 18. Eur Spine J. 2012. PMID: 22526700 Free PMC article.
-
Multiple operations on the same patient.Surg Neurol Int. 2012;3(Suppl 3):S238-43. doi: 10.4103/2152-7806.98578. Epub 2012 Jul 17. Surg Neurol Int. 2012. PMID: 22905330 Free PMC article.
References
-
- Cherkin DC, Deyo RA, Loeser JD, Bush T, Waddell G. An international comparison of back surgery rates. Spine (Phila Pa 1976) 1994;19(11):1201–1206. - PubMed
-
- Davis H. Increasing rates of cervical and lumbar spine surgery in the United States, 1979-1990. Spine (Phila Pa 1976) 1994;19(10):1117–1124. doi: 10.1097/00007632-199405001-00003. Available from: http://dx.doi.org/10.1097/00007632-199405001-00003. - DOI - DOI - PubMed
-
- Deyo RA, Mirza SK, Martin BI, Kreuter W, Goodman DC, Jarvik JG. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA. 2010;303(13):1259–1265. doi: 10.1001/jama.2010.338. Available from: http://dx.doi.org/10.1001/jama.2010.338. - DOI - DOI - PMC - PubMed
-
- Frymoyer JW. Are we performing too much spinal surgery? Iowa Orthop J. 1989;9:32–36.
-
- Frymoyer JW, Pope MH, Clements JH, Wilder DG, MacPherson B, Ashikaga T. Risk factors in low-back pain. An epidemiological survey. J Bone Joint Surg Am. 1983;65(2):213–218. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
