

Review
doi: 10.1007/s00247-011-2012-8.
Epub 2011 Apr 27.
Pulmonary infections
Affiliations
- PMID: 21523569
- PMCID: PMC7079857
- DOI: 10.1007/s00247-011-2012-8
Item in Clipboard
Review
Pulmonary infections
Pediatr Radiol.
2011 May.
Abstract
This paper reviews the most common imaging findings of pulmonary infection in children. Pneumonia is a leading cause of mortality in children in developing and industrialized countries. While the imaging findings usually are nonspecific, correlation with the patient's age, immune status and pertinent history can limit the differential diagnoses. The paper will review the common and unique features of pneumonia caused by specific organisms and in specific patient populations.
Figures
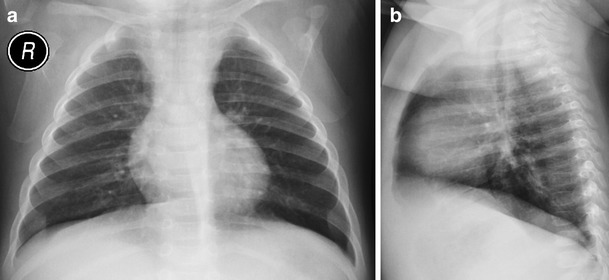
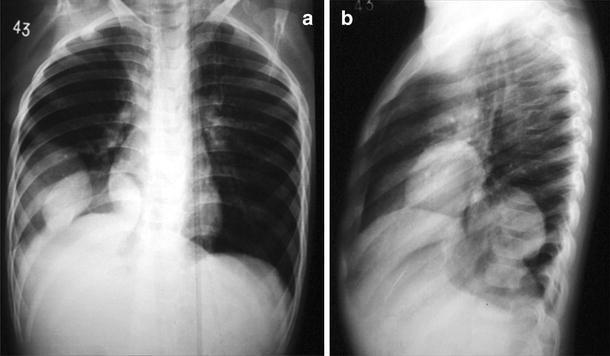
Viral pneumonia in a 13-month-old boy. Frontal (a) and lateral (b) chest radiographs show pulmonary hyperinsufflation with bilateral and symmetrical parahilar opacities
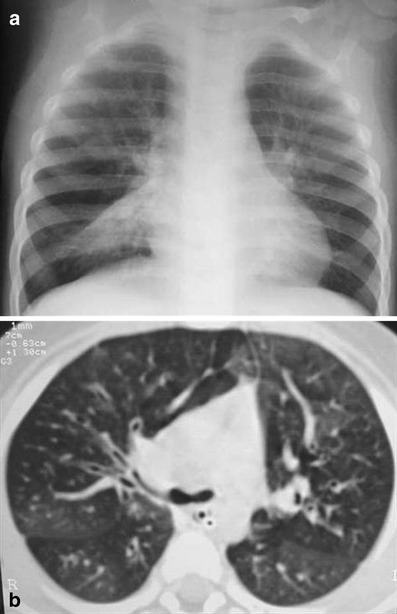
Adenovirus bronchiolitis in an 11-month-old boy. a Chest radiograph demonstrates bilateral pulmonary hyperaeration and right middle lobe atelectasis. b Axial CT shows mosaic attenuation pattern, diffuse cylindrical bronchiectasis and right middle lobe atelectasis
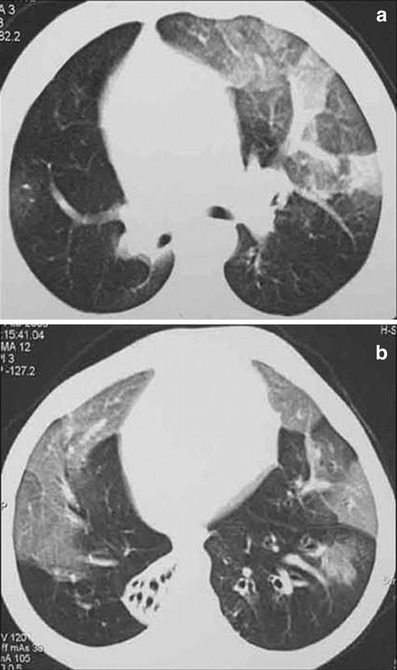
H1N1 infection in a 7-year-old boy. Coronal MPR (a) and axial CT (b) show volume reduction, ground-glass opacities and parenchymal consolidations in the right lung. Left lung shows a mixed pattern of cystic-like hyperinsufflation lesions and ground-glass opacities
Postinfectious bronchiolitis obliterans after adenovirus infection. a, b CT shows extensive bilateral mosaic perfusion pattern with areas of decreased attenuation and vascularity, peribronchial thickening and complete right lower lobe atelectasis
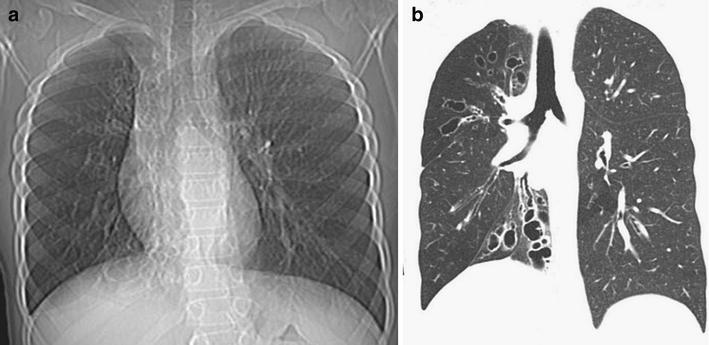
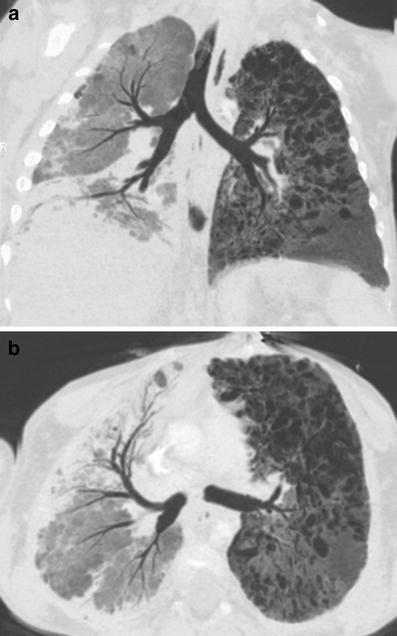
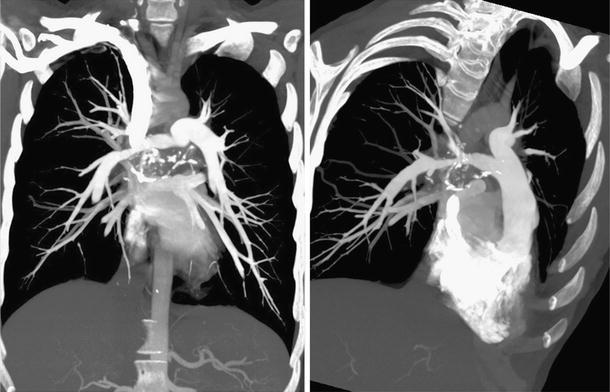
Swyer-James-MacLeod syndrome in an 11-year-old boy. CCR (a) and coronal MPR CT (b) show hyperlucency and decreased vascularity of the right lung. The mediastinum is shifted to the right, consistent with decreased right lung volume. Bronchiectasis is more evident in the upper and lower right lobes
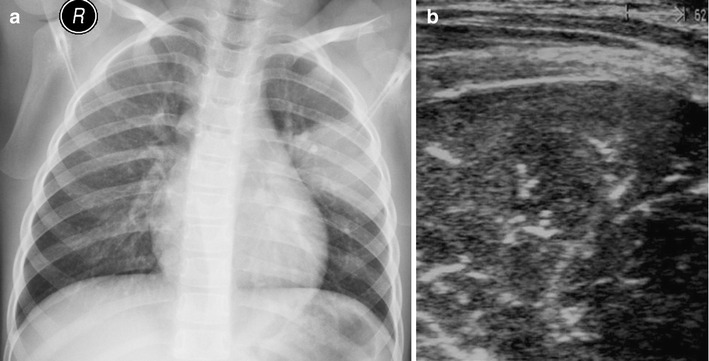
Lobar pneumonia. a Chest radiograph frontal view demonstrates focal area of consolidation in the left upper lobe. b US shows the typical hepatization appearance of lung parenchyma with air bronchograms
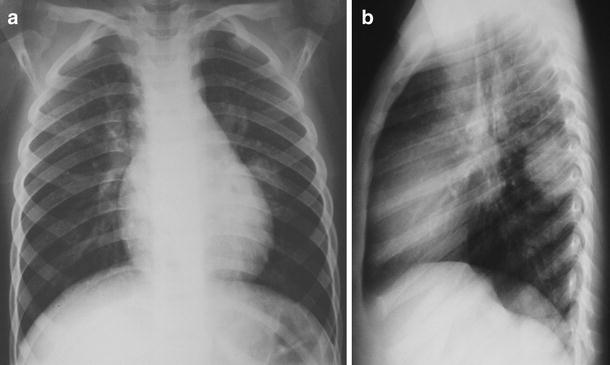
Round pneumonia in a 9-year-old boy. Frontal (a) and lateral (b) chest radiographs show a well-defined mass in the apical segment of the left lower lobe on the lateral view. Chest radiograph obtained 2 weeks later revealed complete resolution
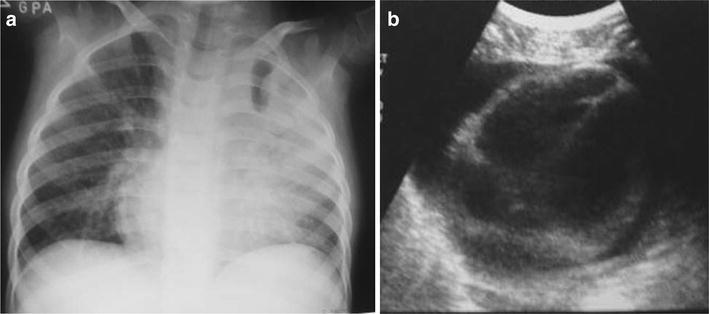
Mycoplasma pneumonia in a 3-year-old girl with low fever and cough. a Frontal chest radiograph shows left upper lobe consolidation. b Pericardial effusion is seen on US image
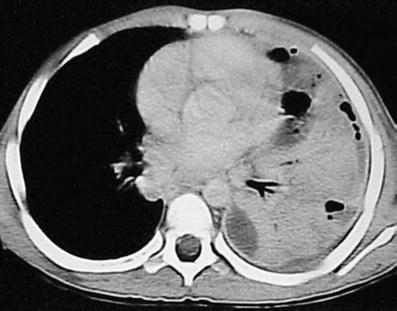
Necrotizing pneumonia. Axial CT after contrast administration shows extensive left lower lobe consolidation with a decreased enhancement area suggesting necrosis. Note the small air-filled cavities
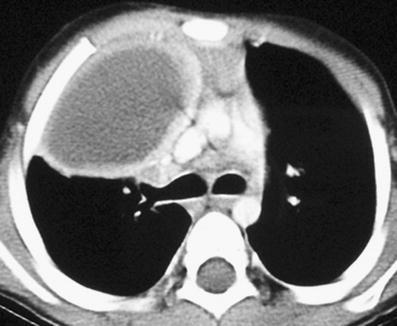
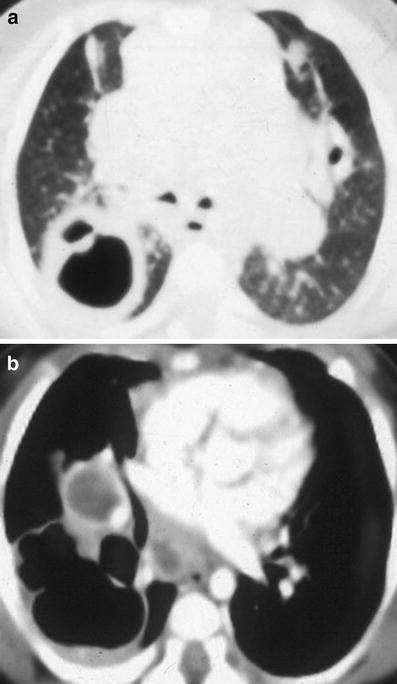
Pulmonary abscess. Contrast-enhanced axial CT of the chest shows a large cavitary lesion in the right upper lobe with a relatively thick wall. The cavity has a smooth inner margin
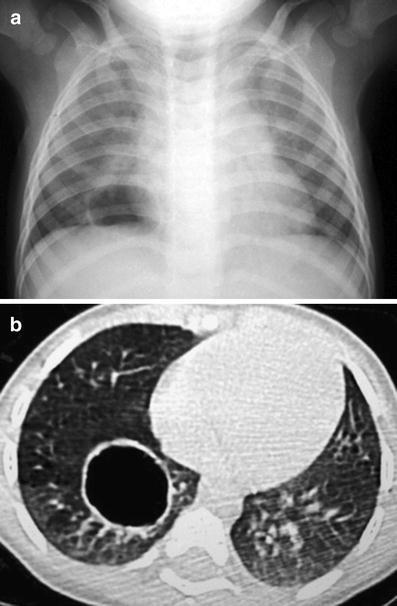
Pneumatocele in an infant. Conventional chest radiograph (a) and axial CT (b) show a thin-walled cavity in the right lower lobe
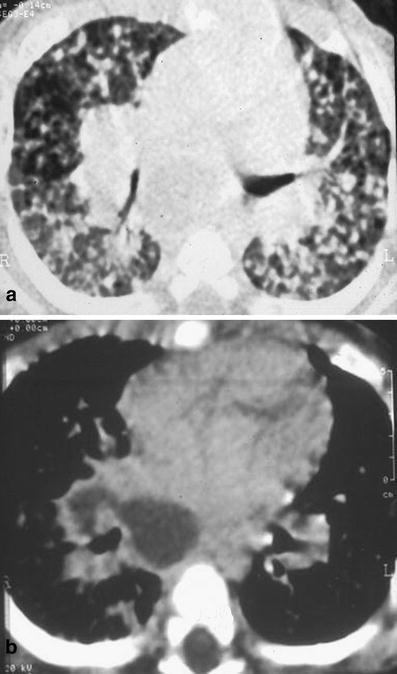
Pulmonary tuberculosis in a 6-month-old boy. Chest CT, lung (a) and mediastinal (b) windows show right hilar lymph node with hypodense center (caseum) and fistulous tract to the main bronchus causing bronchogenic spread, with multiple pulmonary nodules of different sizes in both lungs
Cavitary pulmonary tuberculosis in a 2-month-old boy. Lung (a) and mediastinal (b) axial CT views show a large mediastinal and hilar lymphadenopathy with a cavity lesion in the right lung. Enhanced scan (b) shows cavitary lesion and rim enhancement tuberculosis lymph nodes
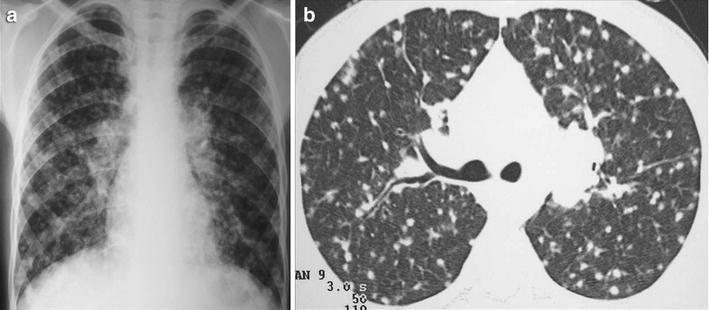
Histoplasmosis in a 9-year-old boy. Chest radiograph (a) and CT (b) show bilateral reticulonodular opacities with multiple diffuse small nodules as well as hilar lymphadenopathies
Fibrosing mediastinitis in a 17-year-old child. CT scan shows a mediastinal mass surrounding and narrowing the right pulmonary artery
Axial CT shows the typical halo sign in an immunocompromised child with invasive aspergillosis
Pulmonary echynococcal cysts. Frontal (a) and lateral (b) chest radiographs show well-defined round masses in the right lower lobe. Chest US (not shown) demonstrated the cystic nature of the lesions
Immunodeficiency. Axial CT shows diffuse bilateral hypoattenuation with decreased vascularity and postinfectious bronchiectasis in a child with IgA deficiency after repeated infections and associated right upper lobe atelectasis
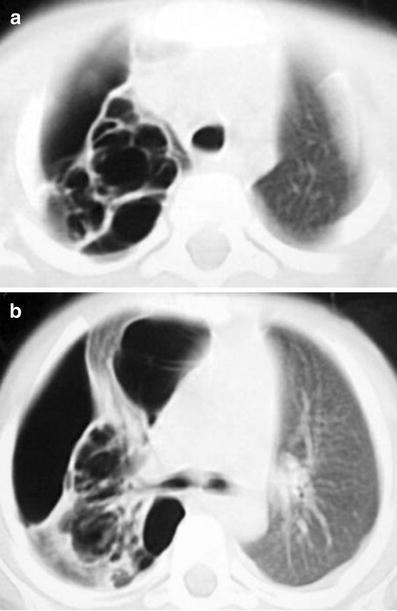
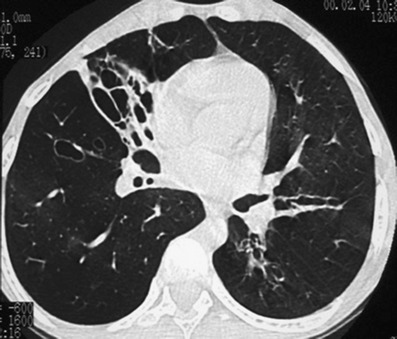
Hyper-IgE syndrome. Axial chest CT (a, b) shows persistent multiple large pneumatoceles, expanding cystic lesions and pneumotorax of right lung
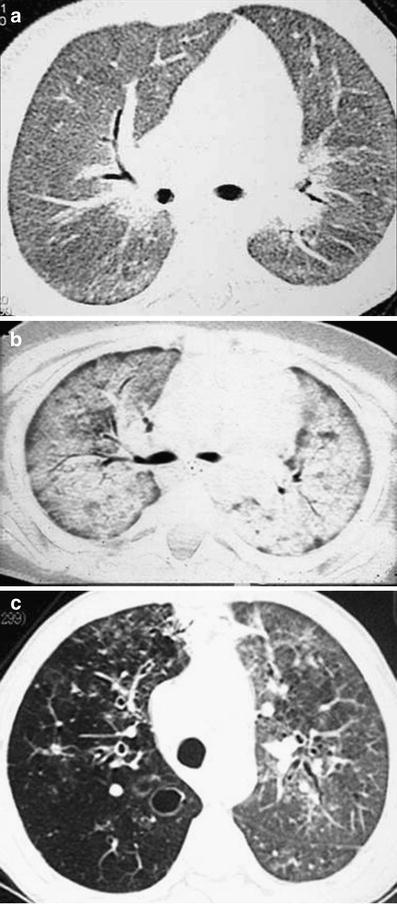
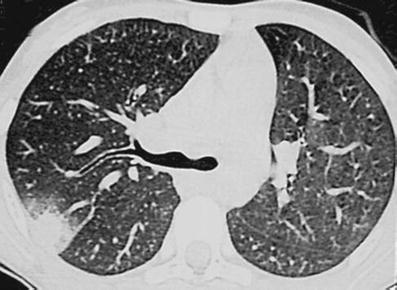
Pneumocystis jirovecii infection. Axial CT views. a Diffuse bilateral reticular interstitial opacities and (b) ground-glass opacities with progressive consolidations from ARDS in two HAART-naïve HIV-positive infants. c An older child with a right hyperlucent lung with small cavitations and incipient bronchiectasis and a left lung with ground-glass pattern after previous recurrent infections

Disseminated cryptococcosis with necrotizing pneumonia and pleural effusion on axial chest CT. This child also had associated meningoencephalitis
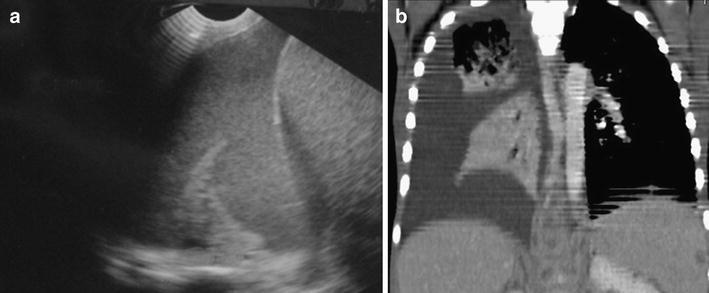
Tuberculosis in a HAART-naïve, HIV-positive 4-year-old girl. a US and (b) coronal MPR CT images show right-side chylothorax caused by erosion of the thoracic duct by several adjacent thoracic-abdominal lymph nodes with intense peripheral enhancement
References
-
- Lucaya J, Strife J. Pediatric chest imaging: chest imaging in infants and children. 3. Berlin: Springer-Verlag; 2002.
-
- Adler B, Effmann E. Pneumonia and pulmonary infection, Chapter 75. In: Slovis TL, editor. Caffey’s pediatric diagnostic imaging. 11. Philadelphia: Mosby; 2008. pp. 1184–1228.
-
- Marks MJ, Haney PJ, McDermott MP, et al. Thoracic disease in children with AIDS. Radiographics. 1996;16:1349–1362. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
