

Disease and host characteristics as predictors of time to first bone metastasis and death in men with progressive castration-resistant nonmetastatic prostate cancer
- PMID: 21523719
- PMCID: PMC3116053
- DOI: 10.1002/cncr.25762
Disease and host characteristics as predictors of time to first bone metastasis and death in men with progressive castration-resistant nonmetastatic prostate cancer
Abstract
Background: The natural history of castration-resistant nonmetastatic prostate cancer is poorly defined.
Methods: The authors used data from 331 subjects in the placebo group of a randomized controlled trial to evaluate the relations of disease and host characteristics with time to first bone metastases in men with prostate cancer, rising prostate-specific antigen (PSA) despite androgen deprivation therapy, and no radiographic evidence of metastases. Relations between baseline covariates and clinical outcomes were assessed by Cox proportional hazard analyses. Covariates in the model were age, body mass index, prior prostatectomy, prior orchiectomy, Gleason score, performance status, PSA, urinary N-telopeptide, bone alkaline phosphatase, albumin, lactate dehydrogenase, and hemoglobin.
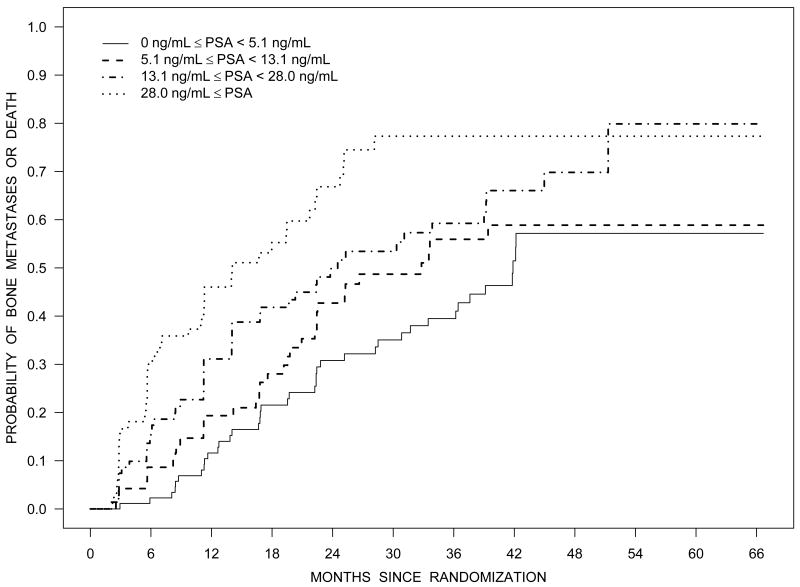
Results: At 2 years, 46% of subjects had developed bone metastases, and 20% had died. Median bone metastasis-free survival was 25 months. In multivariate analyses, baseline PSA ≥ 13.1 ng/mL was associated with shorter overall survival (relative risk [RR], 2.34; 95% confidence interval [CI], 1.71-3.21; P < .0001), time to first bone metastasis (RR, 1.98; 95% CI, 1.43-2.74; P < .0001), and bone metastasis-free survival (RR, 1.98; 95% CI, 1.45-2.70; P < .0001). PSA velocity was significantly associated with overall and bone metastasis-free survival. Other covariates were not consistently associated with clinical outcomes.
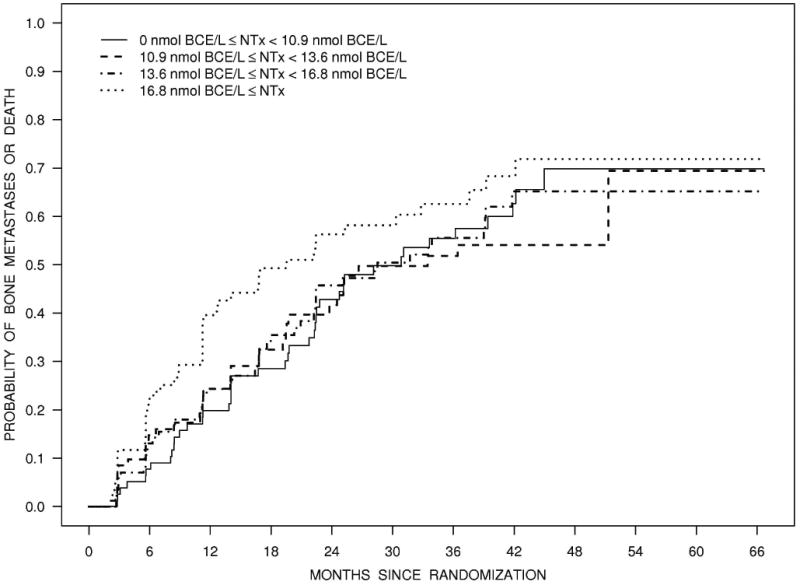
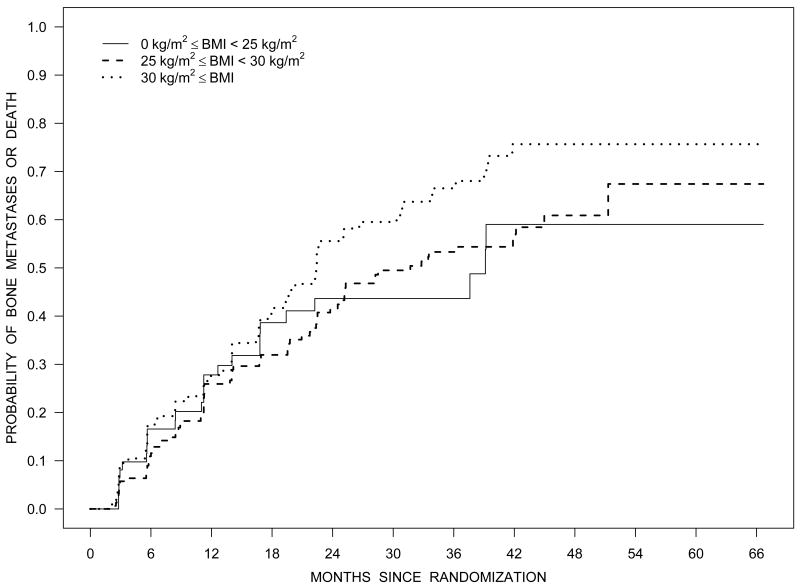
Conclusions: In men with progressive castration-resistant prostate cancer and no detectable metastases, baseline PSA was significantly associated with time to first bone metastasis, bone metastasis-free survival, and overall survival. Other disease and host characteristics, including body mass index and bone turnover markers, were not consistently associated with clinical outcomes.
2010 American Cancer Society.
Figures




References
-
- Petrylak DP, Tangen CM, Hussain MH, et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 2004;351:1513–20. - PubMed
-
- Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351:1502–12. - PubMed
-
- Sharifi N, Gulley JL, Dahut WL. Androgen deprivation therapy for prostate cancer. Jama. 2005;294:238–44. - PubMed
-
- Smith MR, Kabbinavar F, Saad F, et al. Natural history of rising serum prostate-specific antigen in men with castrate nonmetastatic prostate cancer. J Clin Oncol. 2005;23:2918–25. - PubMed
-
- Amling CL, Riffenburgh RH, Sun L, et al. Pathologic variables and recurrence rates as related to obesity and race in men with prostate cancer undergoing radical prostatectomy. J Clin Oncol. 2004;22:439–45. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
