

Myocardial, perivascular, and epicardial fat
- PMID: 21525485
- PMCID: PMC3632210
- DOI: 10.2337/dc11-s250
Myocardial, perivascular, and epicardial fat
Abstract
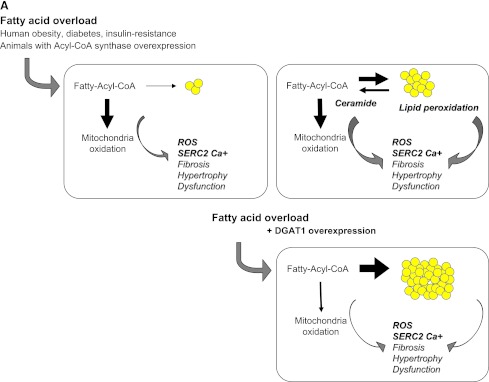
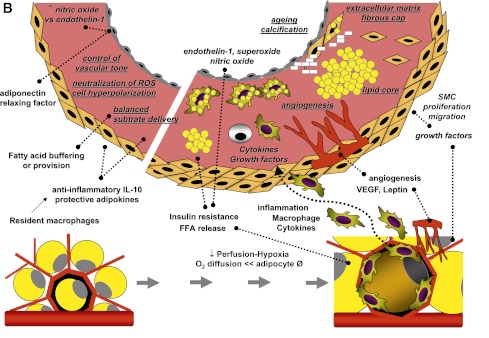
Myocardial fat content refers to the storage of triglyceride droplets within cardiomyocytes. In addition, the heart and arteries are surrounded by layers of adipose tissue, exerting vasocrine and paracrine control of the subtending tissues. The rapid development of the field of noninvasive imaging has made it possible to quantify ectopic fat masses and contents with an increasing degree of accuracy. Myocardial triglyceride stores are increased in obesity, impaired glucose tolerance, and type 2 diabetes. The role of intramyocardial triglyceride accumulation in the pathogenesis of left ventricular (LV) dysfunction remains unclear. Increased triglyceride content is associated with states of fatty acid overload to the heart, saturating the oxidative capacity. It may initially serve as a fatty acid sink to circumscribe the formation of toxic lipid species and subsequently foster cardiac damage. Epicardial and perivascular fat depots may exert a protective modulation of vascular function and energy partition in a healthy situation, but their expansion turns them into an adverse lipotoxic, prothrombotic, and proinflammatory organ. They are augmented in patients with metabolic disorders and coronary artery disease (CAD). However, the progressive association between the quantity of fat and disease severity in terms of extent of plaque calcification or noncalcified areas, markers of plaque vulnerability, and number of vessels involved is less confirmed. Functional or hybrid imaging may contribute to a better definition of disease severity and unveil the direct myocardial and vascular targets of adipose tissue action.
Figures
References
-
- Szczepaniak LS, Dobbins RL, Metzger GJ, et al. Myocardial triglycerides and systolic function in humans: in vivo evaluation by localized proton spectroscopy and cardiac imaging. Magn Reson Med 2003;49:417–423 - PubMed
-
- Taguchi R, Takasu J, Itani Y, et al. Pericardial fat accumulation in men as a risk factor for coronary artery disease. Atherosclerosis 2001;157:203–209 - PubMed
-
- Iacobellis G, Willens HJ. Echocardiographic epicardial fat: a review of research and clinical applications. J Am Soc Echocardiogr 2009;22:1311–1319; quiz 1417–1418 - PubMed
-
- Gorter PM, van Lindert AS, de Vos AM, et al. Quantification of epicardial and peri-coronary fat using cardiac computed tomography; reproducibility and relation with obesity and metabolic syndrome in patients suspected of coronary artery disease. Atherosclerosis 2008;197:896–903 - PubMed
-
- Sacks HS, Fain JN. Human epicardial adipose tissue: a review. Am Heart J 2007;153:907–917 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
