

Do intramedullary spinal cord changes in signal intensity on MRI affect surgical opportunity and approach for cervical myelopathy due to ossification of the posterior longitudinal ligament?
- PMID: 21526380
- PMCID: PMC3175899
- DOI: 10.1007/s00586-011-1813-7
Do intramedullary spinal cord changes in signal intensity on MRI affect surgical opportunity and approach for cervical myelopathy due to ossification of the posterior longitudinal ligament?
Abstract
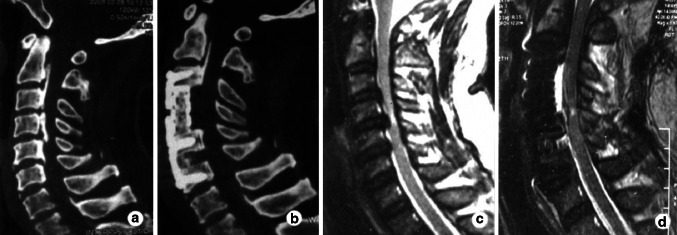
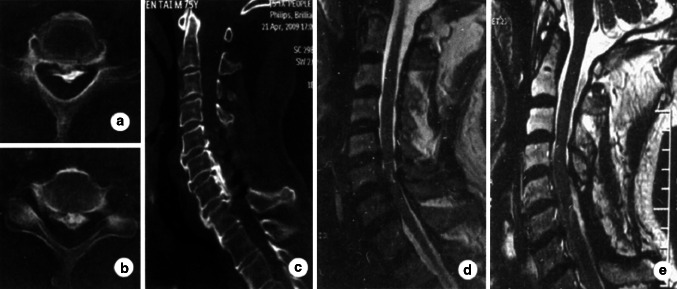
Some controversy still exists over the optimal treatment time and the surgical approach for cervical myelopathy due to ossification of the posterior longitudinal ligament (OPLL). The aim of the current study was first to analyze the effect of intramedullary spinal cord changes in signal intensity (hyperintensity on T2-weighted imaging and hypointensity on T1-weighted imaging) on magnetic resonance imaging (MRI) on surgical opportunity and approach for cervical myelopathy due to OPLL. This was a prospective randomized controlled study. Fifty-six patients with cervical myelopathy due to OPLL were enrolled and assigned to either group A (receiving anterior decompression and fusion, n = 27) or group P (receiving posterior laminectomy, n = 29). All the patients were followed up for an average 20.3 months (12-34 months). The clinical outcomes were assessed by the average operative time, blood loss, Japanese Orthopedic Association (JOA) score, improvement rate (IR) and complication. To determine the relevant statistics, we made two factorial designs and regrouped the data of all patients to group H (with hyperintensity on MRI, n = 31), group L (with hypointensity on MRI, n = 19) and group N (no signal on MRI, n = 25), and then to further six subgroups as well: AH (with hyperintensity on MRI from group A, n = 15), PH (with hyperintensity on MRI from group P, n = 16), AL (with hypointensity on MRI from group A, n = 10), PL (with hypointensity on MRI from group P, n = 9), AN (no signal intensity on MRI from group A, n = 12) and PN (no signal intensity on MRI from group P, n = 13). Both hyperintensity on T2-weighted imaging and hypointensity on T1-weighted imaging had a close relationship with the JOA score and IR. The pre- and postoperative JOA score and postoperative IR of either group H or group L was significantly lower than that of group N (P < 0.05), regardless of whether the patients had received anterior or posterior surgery. On the other hand, both the JOA score and IR of subgroup AH were higher than those of subgroup PH at 1 week, 6 and 12 months postoperatively (P < 0.05), as well as between subgroup AL and PL; but in group N, there was no difference between the subgroup AN and PN (P > 0.05). In conclusion, regardless of hyperintensity on T2-weighted imaging or hypointensity on T1-weighted imaging in patients with OPLL, severe damage to the spinal cord is indicated. Surgical treatment should be provided before the advent of intramedullary spinal cord changes in signal intensity on MRI. The anterior approach is more effective than posterior approach for treating cervical myelopathy due to OPLL characterized by intramedullary spinal cord changes in signal intensity on MRI.
Figures
References
-
- Epstein N (2002) Posterior approaches in the management of cervical spondylosis and ossification of the posterior longitudinal ligament. Surg Neurol 58:194–207 (discussion 207–208) - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
