

SNP array-based karyotyping: differences and similarities between aplastic anemia and hypocellular myelodysplastic syndromes
- PMID: 21527527
- PMCID: PMC3128479
- DOI: 10.1182/blood-2010-11-314393
SNP array-based karyotyping: differences and similarities between aplastic anemia and hypocellular myelodysplastic syndromes
Abstract
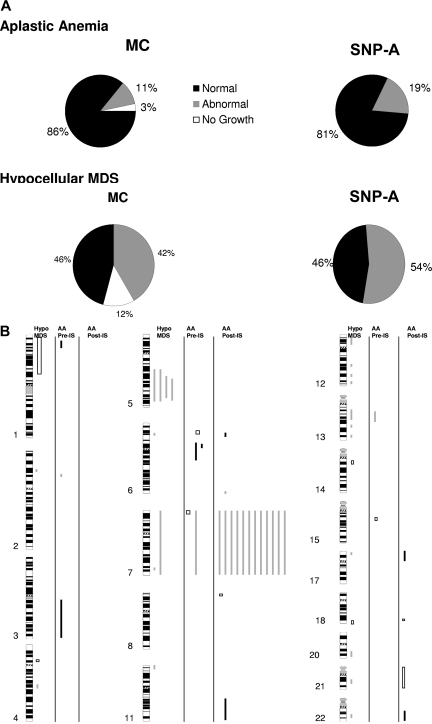
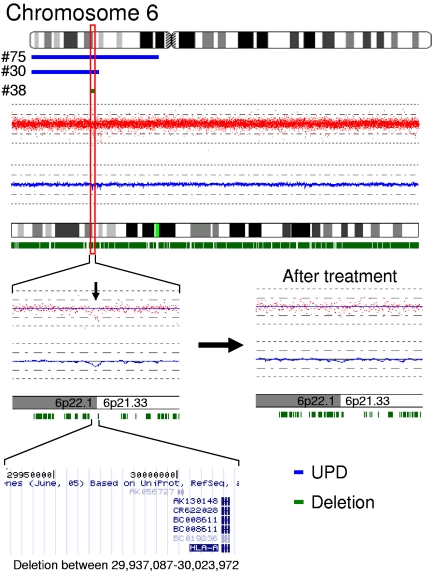
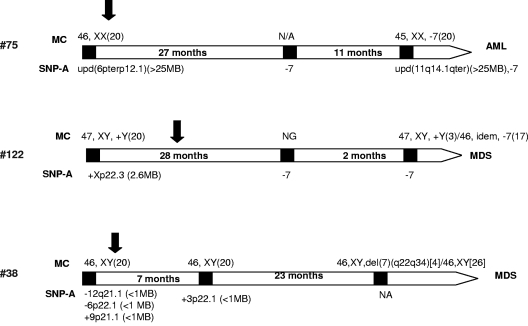
In aplastic anemia (AA), contraction of the stem cell pool may result in oligoclonality, while in myelodysplastic syndromes (MDS) a single hematopoietic clone often characterized by chromosomal aberrations expands and outcompetes normal stem cells. We analyzed patients with AA (N = 93) and hypocellular MDS (hMDS, N = 24) using single nucleotide polymorphism arrays (SNP-A) complementing routine cytogenetics. We hypothesized that clinically important cryptic clonal aberrations may exist in some patients with BM failure. Combined metaphase and SNP-A karyotyping improved detection of chromosomal lesions: 19% and 54% of AA and hMDS cases harbored clonal abnormalities including copy-neutral loss of heterozygosity (UPD, 7%). Remarkably, lesions involving the HLA locus suggestive of clonal immune escape were found in 3 of 93 patients with AA. In hMDS, additional clonal lesions were detected in 5 (36%) of 14 patients with normal/noninformative routine cytogenetics. In a subset of AA patients studied at presentation, persistent chromosomal genomic lesions were found in 10 of 33, suggesting that the initial diagnosis may have been hMDS. Similarly, using SNP-A, earlier clonal evolution was found in 4 of 7 AA patients followed serially. In sum, our results indicate that SNP-A identify cryptic clonal genomic aberrations in AA and hMDS leading to improved distinction of these disease entities.
Figures

References
-
- Mufti GJ. Chromosomal deletions in the myelodysplastic syndrome. Leuk Res. 1992;16(1):35–41. - PubMed
-
- Fenaux P. Chromosome and molecular abnormalities in myelodysplastic syndromes. Int J Hematol. 2001;73(4):429–437. - PubMed
-
- Barrett J, Saunthararajah Y, Molldrem J. Myelodysplastic syndrome and aplastic anemia: distinct entities or diseases linked by a common pathophysiology? Semin Hematol. 2000;37(1):15–29. - PubMed
-
- Toyama K, Ohyashiki K, Yoshida Y, et al. Clinical and cytogenetic findings of myelodysplastic syndromes showing hypocellular bone marrow or minimal dysplasia, in comparison with typical myelodysplastic syndromes. Int J Hematol. 1993;58(1–2):53–61. - PubMed
-
- Maciejewski JP, Risitano A, Sloand EM, Nunez O, Young NS. Distinct clinical outcomes for cytogenetic abnormalities evolving from aplastic anemia. Blood. 2002;99(9):3129–3135. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
