

Prospective analysis of parametric response map-derived MRI biomarkers: identification of early and distinct glioma response patterns not predicted by standard radiographic assessment
- PMID: 21527563
- PMCID: PMC3139775
- DOI: 10.1158/1078-0432.CCR-10-2098
Prospective analysis of parametric response map-derived MRI biomarkers: identification of early and distinct glioma response patterns not predicted by standard radiographic assessment
Abstract
Purpose: Currently, radiologic response of brain tumors is assessed according to the Macdonald criteria 10 weeks from the start of therapy. There exists a critical need to identify nonresponding patients early in the course of their therapy for consideration of alternative treatment strategies. Our study assessed the effectiveness of the parametric response map (PRM) imaging biomarker to provide for an earlier measure of patient survival prediction.
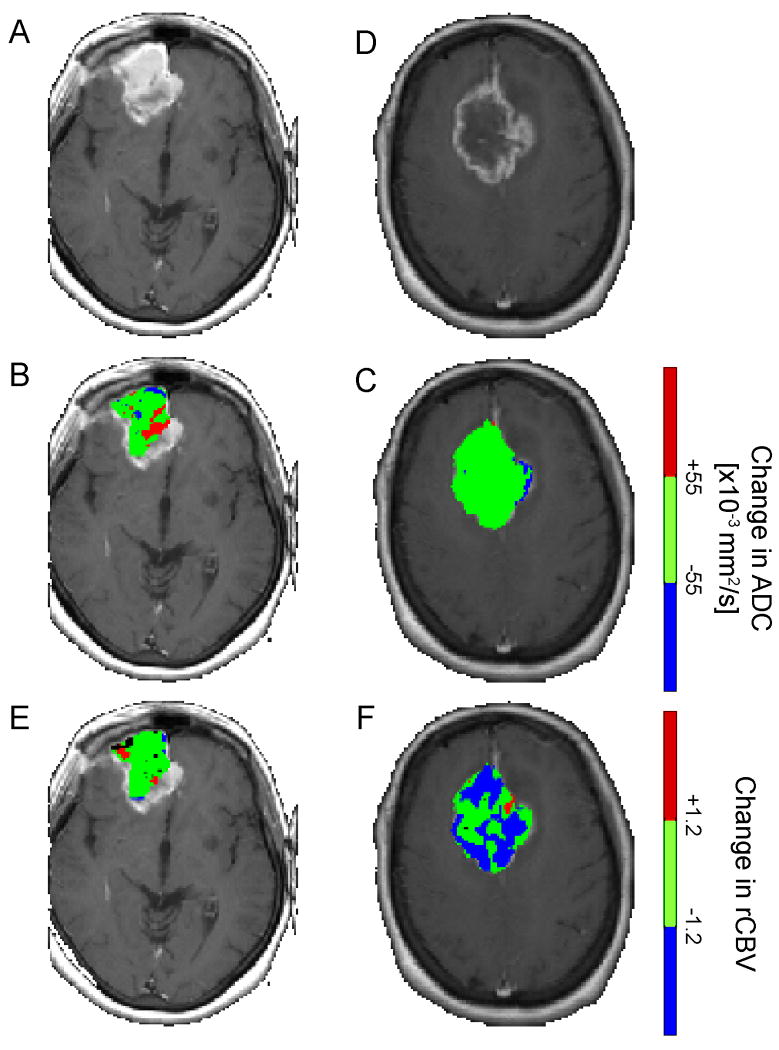
Experimental design: Forty-five high-grade glioma patients received concurrent chemoradiation. Quantitative MRI including apparent diffusion coefficient (ADC) and relative cerebral blood volume (rCBV) maps were acquired pretreatment and 3 weeks midtreatment on a prospective institutional-approved study. PRM, a voxel-by-voxel image analysis method, was evaluated as an early prognostic biomarker of overall survival. Clinical and conventional MR parameters were also evaluated.
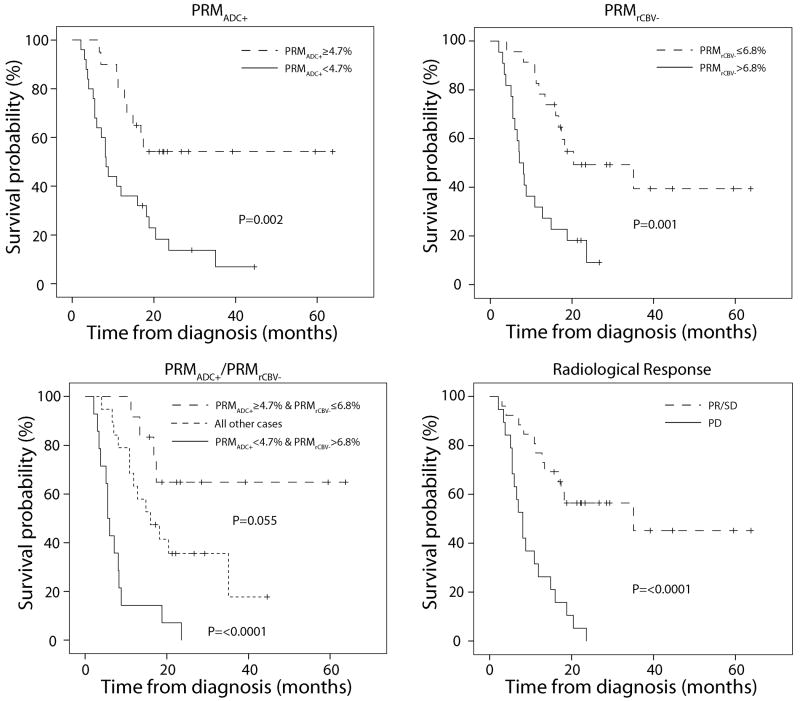
Results: Multivariate analysis showed that PRM(ADC+) in combination with PRM(rCBV-) obtained at week 3 had a stronger correlation to 1-year and overall survival rates than any baseline clinical or treatment response imaging metric. The composite biomarker identified three distinct patient groups, nonresponders [median survival (MS) of 5.5 months, 95% CI: 4.4-6.6 months], partial responders (MS of 16 months, 95% CI: 8.6-23.4 months), and responders (MS has not yet been reached).
Conclusions: Inclusion of PRM(ADC+) and PRM(rCBV-) into a single imaging biomarker metric provided early identification of patients resistant to standard chemoradiation. In comparison to the current standard of assessment of response at 10 weeks (Macdonald criteria), the composite PRM biomarker potentially provides a useful opportunity for clinicians to identify patients who may benefit from alternative treatment strategies.
Figures
References
-
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–66. - PubMed
-
- Macdonald DR, Cascino TL, Schold SC, Jr, Cairncross JG. Response criteria for phase II studies of supratentorial malignant glioma. J Clin Oncol. 1990;8:1277–80. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–96. - PubMed
-
- Wen PY, Macdonald DR, Reardon DA, Cloughesy TF, Sorensen AG, Galanis E, et al. Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J Clin Oncol. 2010;28:1963–72. - PubMed
-
- Stupp R, Hegi ME, Neyns B, Goldbrunner R, Schlegel U, Clement PM, et al. Phase I/IIa study of cilengitide and temozolomide with concomitant radiotherapy followed by cilengitide and temozolomide maintenance therapy in patients with newly diagnosed glioblastoma. J Clin Oncol. 2010;28:2712–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
