

Predictive factors of clinical response in steroid-refractory ulcerative colitis treated with granulocyte-monocyte apheresis
- PMID: 21528055
- PMCID: PMC3080717
- DOI: 10.3748/wjg.v17.i14.1831
Predictive factors of clinical response in steroid-refractory ulcerative colitis treated with granulocyte-monocyte apheresis
Abstract
Aim: To identify factors predicting the clinical response of ulcerative colitis patients to granulocyte-monocyte apheresis (GMA).
Methods: Sixty-nine ulcerative colitis patients (39 F, 30 M) dependent upon/refractory to steroids were treated with GMA. Steroid dependency, clinical activity index (CAI), C reactive protein (CRP) level, erythrocyte sedimentation rate (ESR), values at baseline, use of immunosuppressant, duration of disease, and age and extent of disease were considered for statistical analysis as predictive factors of clinical response. Univariate and multivariate logistic regression models were used.
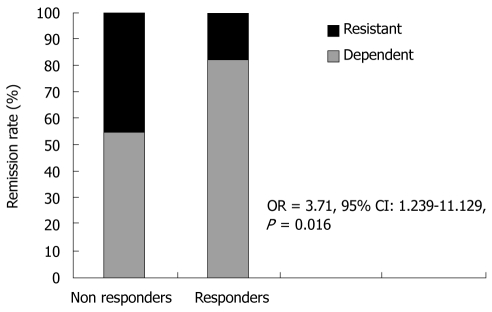
Results: In the univariate analysis, CAI (P = 0.039) and ESR (P = 0.017) levels at baseline were singled out as predictive of clinical remission. In the multivariate analysis steroid dependency [Odds ratio (OR) = 0.390, 95% Confidence interval (CI): 0.176-0.865, Wald 5.361, P = 0.0160] and low CAI levels at baseline (4 < CAI < 7) (OR = 0.770, 95% CI: 0.425-1.394, Wald 3.747, P = 0.028) proved to be effective as factors predicting clinical response.
Conclusion: GMA may be a valid therapeutic option for steroid-dependent ulcerative colitis patients with mild-moderate disease and its clinical efficacy seems to persist for 12 mo.
Keywords: Granulocyte-monocyte apheresis; Long-term follow-up; Predictive factors; Steroid therapy; Ulcerative colitis.
Figures
References
-
- Podolsky DK. Inflammatory bowel disease. N Engl J Med. 2002;347:417–429. - PubMed
-
- Faubion WA Jr, Loftus EV Jr, Harmsen WS, Zinsmeister AR, Sandborn WJ. The natural history of corticosteroid therapy for inflammatory bowel disease: a population-based study. Gastroenterology. 2001;121:255–260. - PubMed
-
- Masunaga Y, Ohno K, Ogawa R, Hashiguchi M, Echizen H, Ogata H. Meta-analysis of risk of malignancy with immunosuppressive drugs in inflammatory bowel disease. Ann Pharmacother. 2007;41:21–28. - PubMed
-
- Cohen RD. Efficacy and safety of repeated infliximab infusions for Crohn's disease: 1-year clinical experience. Inflamm Bowel Dis. 2001;7 Suppl 1:S17–S22. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
