

The mucocutaneous and systemic phenotype of dermatomyositis patients with antibodies to MDA5 (CADM-140): a retrospective study
- PMID: 21531040
- PMCID: PMC3167687
- DOI: 10.1016/j.jaad.2010.09.016
The mucocutaneous and systemic phenotype of dermatomyositis patients with antibodies to MDA5 (CADM-140): a retrospective study
Abstract
Background: Dermatomyositis (DM) is a multisystem autoimmune disease, in which serologic evidence of immune responses to disease-specific antigenic targets is found in approximately 50% to 70% of patients. Recently, melanoma differentiation-associated gene 5 (MDA5) has been identified as a DM-specific autoantigen that appears to be targeted in patients with DM and mild or absent muscle inflammation and with an increased risk of interstitial lung disease.
Objective: We wished to understand the role of MDA5 in DM skin inflammation by testing it to determine if a specific cutaneous phenotype is associated with MDA5 reactivity.
Methods: We retrospectively screened plasma from 77 patients with DM in the outpatient clinics at the Stanford University Department of Dermatology in California.
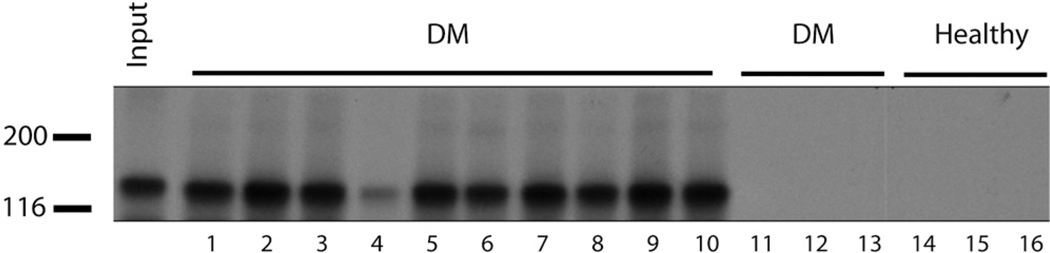
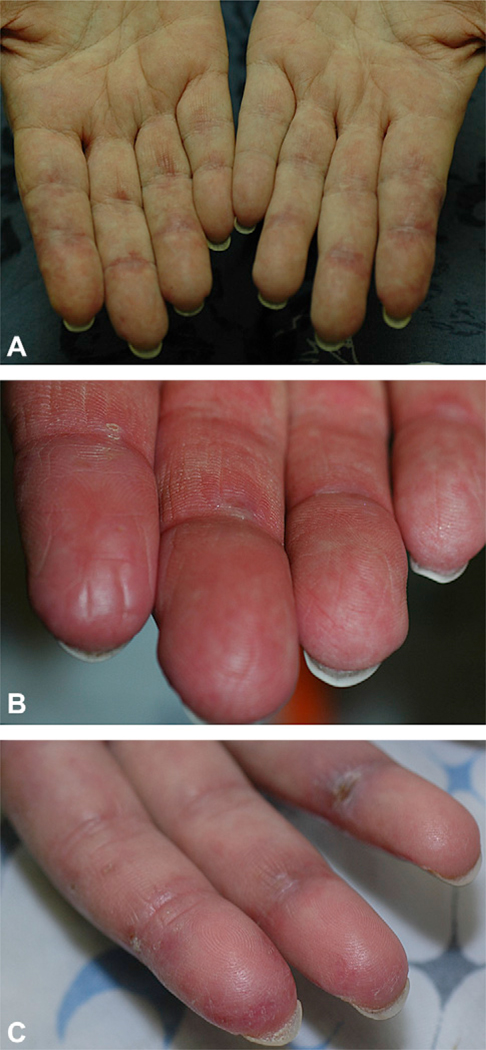
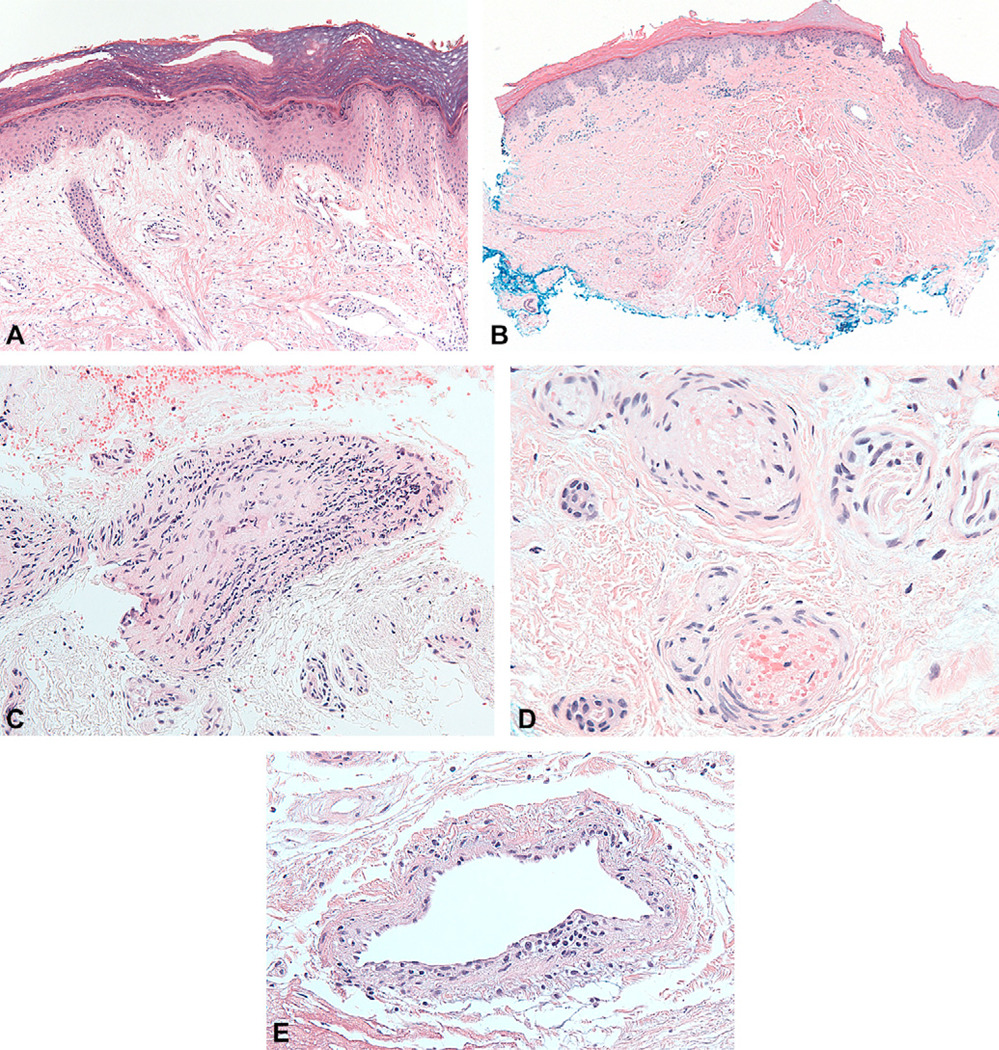
Results: We found that 10 (13%) patients had circulating anti-MDA5 antibodies, and had a characteristic cutaneous phenotype consisting of skin ulceration, tender palmar papules, or both. Typical areas of skin ulceration included the lateral nailfolds, Gottron papules, and elbows. Biopsy specimens of the palmar papules showed a vasculopathy characterized by vascular fibrin deposition with variable perivascular inflammation. Patients with anti-MDA5 antibodies also had an increased risk of oral pain and/or ulceration, hand swelling, arthritis/arthralgia, and diffuse hair loss. Consistent with previous reports, these patients had little or no myositis and had increased risk of interstitial lung disease.
Limitations: This study was conducted at a tertiary referral center. Multiple associations with MDA5 antibodies were tested retrospectively on a relatively small cohort of 10 anti-MDA5-positive patients.
Conclusion: We suggest that MDA5 reactivity in DM characterizes a patient population with severe vasculopathy.
Copyright © 2010 American Academy of Dermatology, Inc. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest: None declared.
Figures

References
-
- Gunawardena H, Betteridge ZE, McHugh NJ. Myositis-specific autoantibodies: their clinical and pathogenic significance in disease expression. Rheumatology (Oxford) 2009;48:607–612. - PubMed
-
- Levine SM, Raben N, Xie D, Askin FB, Tuder R, Mullins M, et al. Novel conformation of histidyl-transfer RNA synthetase in the lung: the target tissue in Jo-1 autoantibody-associated myositis. Arthritis Rheum. 2007;56:2729–2739. - PubMed
-
- Caproni M, Torchia D, Cardinali C, Volpi W, Del Bianco E, D’Agata A, et al. Infiltrating cells, related cytokines and chemokine receptors in lesional skin of patients with dermatomyositis. Br J Dermatol. 2004;151:784–791. - PubMed
-
- Magro CM, Segal JP, Crowson AN, Chadwick P. The phenotypic profile of dermatomyositis and lupus erythematosus: a comparative analysis. J Cutan Pathol. 2010;37:659–671. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
