

Gatifloxacin versus chloramphenicol for uncomplicated enteric fever: an open-label, randomised, controlled trial
- PMID: 21531174
- PMCID: PMC3108101
- DOI: 10.1016/S1473-3099(11)70089-5
Gatifloxacin versus chloramphenicol for uncomplicated enteric fever: an open-label, randomised, controlled trial
Abstract
Background: We aimed to investigate whether gatifloxacin, a new generation and affordable fluoroquinolone, is better than chloramphenicol for the treatment of uncomplicated enteric fever in children and adults.
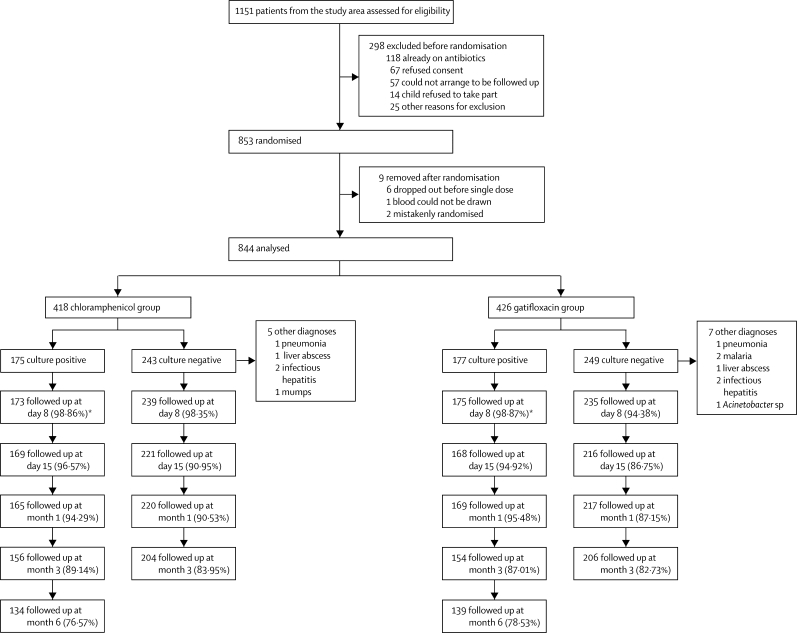
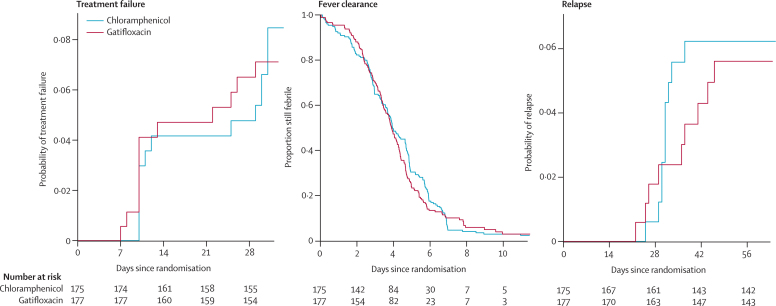
Methods: We did an open-label randomised superiority trial at Patan Hospital, Kathmandu, Nepal, to investigate whether gatifloxacin is more effective than chloramphenicol for treating uncomplicated enteric fever. Children and adults clinically diagnosed with enteric fever received either gatifloxacin (10 mg/kg) once a day for 7 days, or chloramphenicol (75 mg/kg per day) in four divided doses for 14 days. Patients were randomly allocated treatment (1:1) in blocks of 50, without stratification. Allocations were placed in sealed envelopes opened by the study physician once a patient was enrolled into the trial. Masking was not possible because of the different formulations and ways of giving the two drugs. The primary outcome measure was treatment failure, which consisted of at least one of the following: persistent fever at day 10, need for rescue treatment, microbiological failure, relapse until day 31, and enteric-fever-related complications. The primary outcome was assessed in all patients randomly allocated treatment and reported separately for culture-positive patients and for all patients. Secondary outcome measures were fever clearance time, late relapse, and faecal carriage. The trial is registered on controlled-trials.com, number ISRCTN 53258327.
Findings: 844 patients with a median age of 16 (IQR 9-22) years were enrolled in the trial and randomly allocated a treatment. 352 patients had blood-culture-confirmed enteric fever: 175 were treated with chloramphenicol and 177 with gatifloxacin. 14 patients had treatment failure in the chloramphenicol group, compared with 12 in the gatifloxacin group (hazard ratio [HR] of time to failure 0·86, 95% CI 0·40-1·86, p=0·70). The median time to fever clearance was 3·95 days (95% CI 3·68-4·68) in the chloramphenicol group and 3·90 days (3·58-4·27) in the gatifloxacin group (HR 1·06, 0·86-1·32, p=0·59). At 1 month only, three of 148 patients were stool-culture positive in the chloramphenicol group and none in the gatifloxacin group. At the end of 3 months only one person had a positive stool culture in the chloramphenicol group. There were no other positive stool cultures even at the end of 6 months. Late relapses were noted in three of 175 patients in the culture-confirmed chloramphenicol group and two of 177 in the gatifloxacin group. There were no culture-positive relapses after day 62. 99 patients (24%) experienced 168 adverse events in the chloramphenicol group and 59 (14%) experienced 73 events in the gatifloxacin group.
Interpretation: Although no more efficacious than chloramphenicol, gatifloxacin should be the preferred treatment for enteric fever in developing countries because of its shorter treatment duration and fewer adverse events.
Funding: Wellcome Trust.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Outpatient treatment of patients with enteric fever.Lancet Infect Dis. 2011 Jun;11(6):419-21. doi: 10.1016/S1473-3099(11)70119-0. Epub 2011 Apr 29. Lancet Infect Dis. 2011. PMID: 21531173 No abstract available.
-
Multidrug-resistant Salmonella enterica.Lancet Infect Dis. 2011 Nov;11(11):808-9. doi: 10.1016/S1473-3099(11)70299-7. Lancet Infect Dis. 2011. PMID: 22035610 No abstract available.
References
-
- Parry CM, Hien TT, Dougan G, White NJ, Farrar JJ. Typhoid fever. N Engl J Med. 2002;347:1770–1782. - PubMed
-
- Bhan MK, Bahl R, Bhatnagar S. Typhoid and paratyphoid fever. Lancet. 2005;366:749–762. - PubMed
-
- Woodward TE, Smadel JE, Ley HL, Green R, Mankikar DS. Preliminary report on the beneficial effect of chloromycetin in the treatment of typhoid fever. Ann Intern Med. 1948;29:131–134. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
