

Triglyceride-rich lipoproteins and high-density lipoprotein cholesterol in patients at high risk of cardiovascular disease: evidence and guidance for management
- PMID: 21531743
- PMCID: PMC3105250
- DOI: 10.1093/eurheartj/ehr112
Triglyceride-rich lipoproteins and high-density lipoprotein cholesterol in patients at high risk of cardiovascular disease: evidence and guidance for management
Abstract
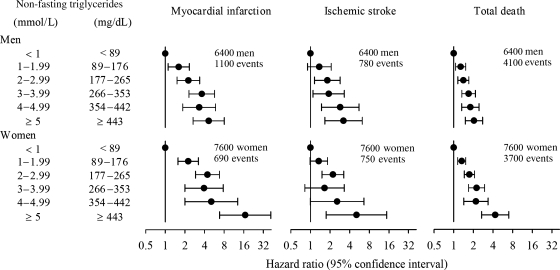
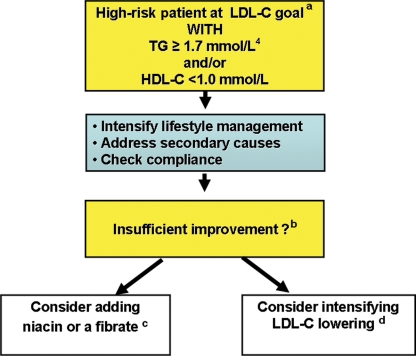
Even at low-density lipoprotein cholesterol (LDL-C) goal, patients with cardiometabolic abnormalities remain at high risk of cardiovascular events. This paper aims (i) to critically appraise evidence for elevated levels of triglyceride-rich lipoproteins (TRLs) and low levels of high-density lipoprotein cholesterol (HDL-C) as cardiovascular risk factors, and (ii) to advise on therapeutic strategies for management. Current evidence supports a causal association between elevated TRL and their remnants, low HDL-C, and cardiovascular risk. This interpretation is based on mechanistic and genetic studies for TRL and remnants, together with the epidemiological data suggestive of the association for circulating triglycerides and cardiovascular disease. For HDL, epidemiological, mechanistic, and clinical intervention data are consistent with the view that low HDL-C contributes to elevated cardiovascular risk; genetic evidence is unclear however, potentially reflecting the complexity of HDL metabolism. The Panel believes that therapeutic targeting of elevated triglycerides (≥ 1.7 mmol/L or 150 mg/dL), a marker of TRL and their remnants, and/or low HDL-C (<1.0 mmol/L or 40 mg/dL) may provide further benefit. The first step should be lifestyle interventions together with consideration of compliance with pharmacotherapy and secondary causes of dyslipidaemia. If inadequately corrected, adding niacin or a fibrate, or intensifying LDL-C lowering therapy may be considered. Treatment decisions regarding statin combination therapy should take into account relevant safety concerns, i.e. the risk of elevation of blood glucose, uric acid or liver enzymes with niacin, and myopathy, increased serum creatinine and cholelithiasis with fibrates. These recommendations will facilitate reduction in the substantial cardiovascular risk that persists in patients with cardiometabolic abnormalities at LDL-C goal.
Figures
References
-
- European Cardiovascular Disease Statistics. 2008. http://www.heartstats.org/datapage.asp?id=7683. (2 November 2010)
-
- Annual Report of the EHN activities and its members in 2008. http://www.ehnheart.org/publications/annual-reports.html. (28 May 2010)
-
- Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87:4–14. - PubMed
-
- Graham I, Atar D, Borch-Johnsen K, Boysen G, Burell G, Cifkova R, Dallongeville J, De Backer G, Ebrahim S, Gjelsvik B, Herrmann-Lingen C, Hoes A, Humphries S, Knapton M, Perk J, Priori SG, Pyorala K, Reiner Z, Ruilope L, Sans-Menendez S, Scholte op Reimer W, Weissberg P, Wood D, Yarnell J, Zamorano JL, Walma E, Fitzgerald T, Cooney MT, Dudina A European Society of Cardiology (ESC) Committee for Practice Guidelines (CPG) European guidelines on cardiovascular disease prevention in clinical practice: executive summary: Fourth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (Constituted by representatives of nine societies and by invited experts) Eur Heart J. 2007;28:2375–2414. - PubMed
-
- Grundy SM, Cleeman JI, Merz CN, Brewer HB, Jr, Clark LT, Hunninghake DB, Pasternak RC, Smith SC, Jr, Stone NJ Coordinating Committee of the National Cholesterol Education Program. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. Arterioscler Thromb Vasc Biol. 2004;24:e149–e161. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
