

A role for interleukin-2 trans-presentation in dendritic cell-mediated T cell activation in humans, as revealed by daclizumab therapy
- PMID: 21532597
- PMCID: PMC3089658
- DOI: 10.1038/nm.2365
A role for interleukin-2 trans-presentation in dendritic cell-mediated T cell activation in humans, as revealed by daclizumab therapy
Abstract
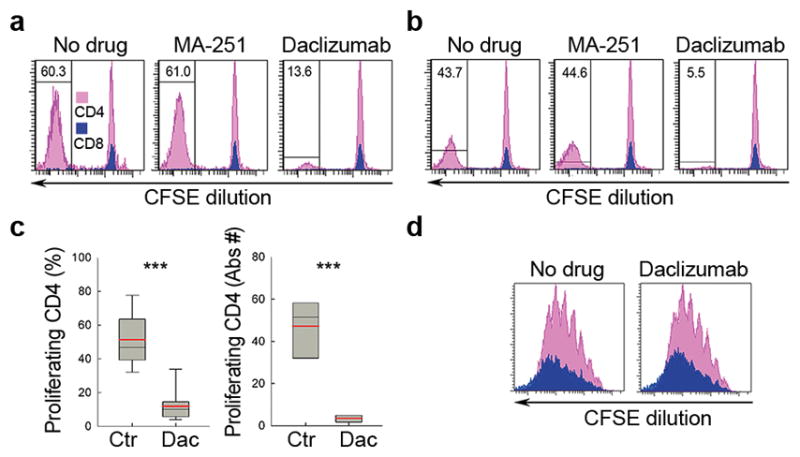
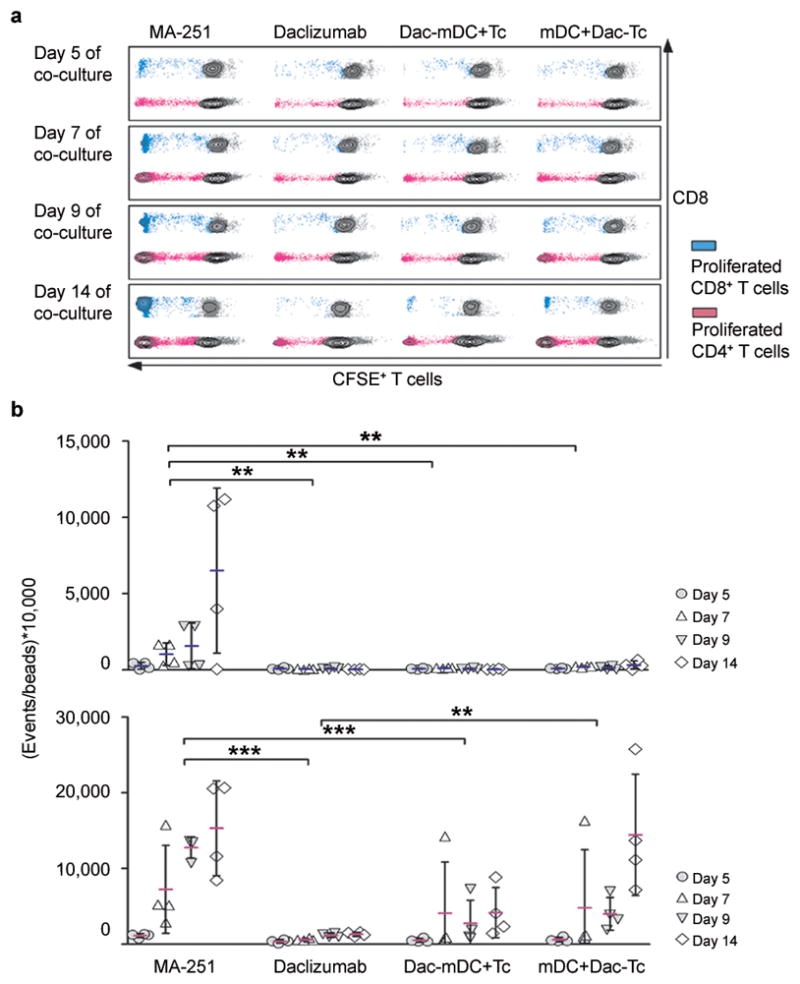
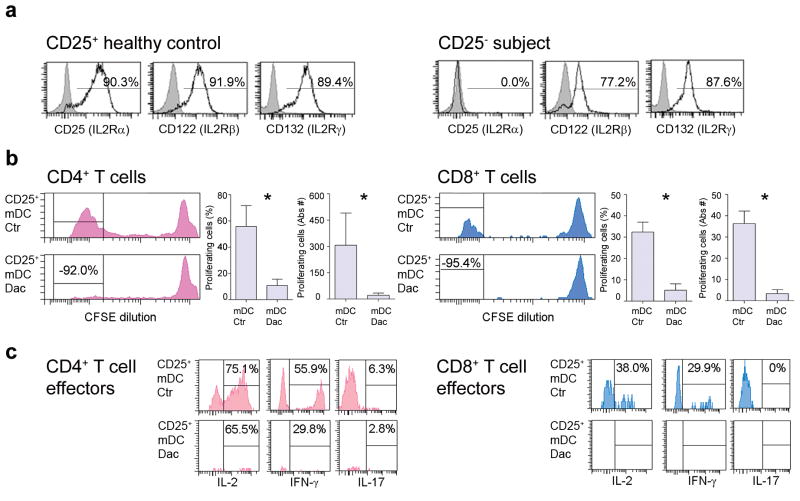
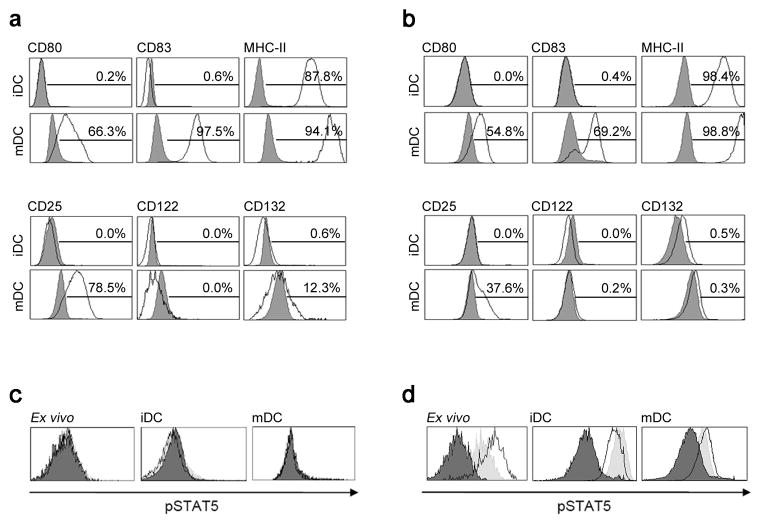
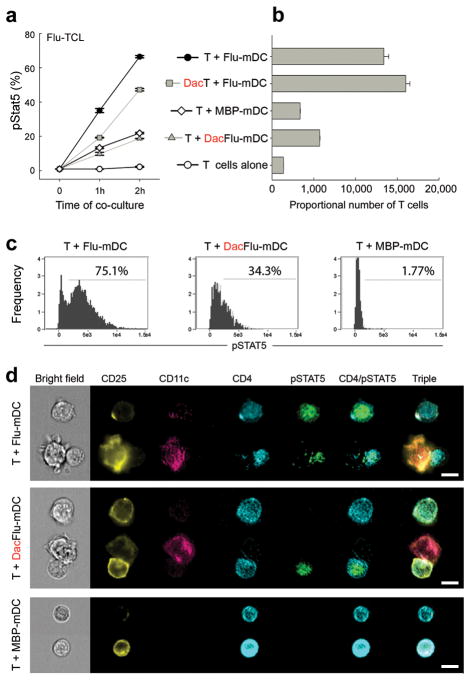
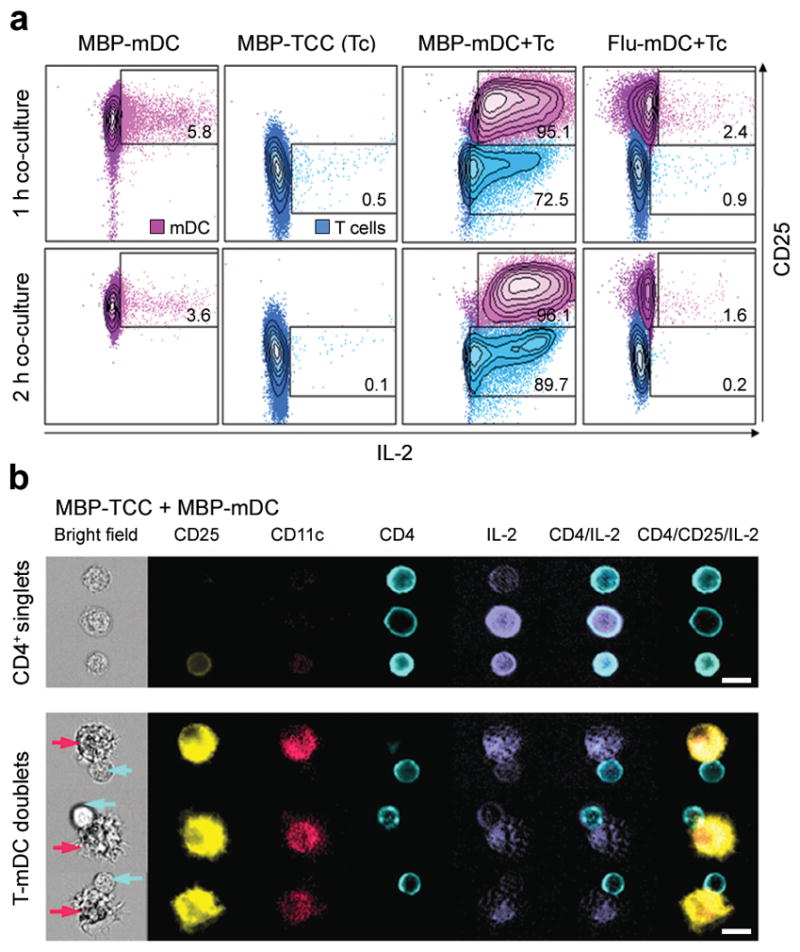
Although previous studies have described CD25 expression and production of interleukin-2 (IL-2) by mature dendritic cells (mDCs), it remains unclear how these molecules participate in the activation of T cells. In search of the mechanisms by which daclizumab, a humanized monoclonal antibody against CD25, inhibits brain inflammation in multiple sclerosis, we observed that although the drug has limited effects on polyclonal T cell activation, it potently inhibits activation of antigen-specific T cells by mDCs. We show that mDCs (and antigen-experienced T cells) secrete IL-2 toward the mDC-T cell interface in an antigen-specific manner, and mDCs 'lend' their CD25 to primed T cells in trans to facilitate early high-affinity IL-2 signaling, which is crucial for subsequent T cell expansion and development of antigen-specific effectors. Our data reveal a previously unknown mechanism for the IL-2 receptor system in DC-mediated activation of T cells.
Conflict of interest statement
B.B. and T.A.W. are co-inventors on NIH patents related to the use of daclizumab in MS and as such have received patent royalty payments.
Figures
Comment in
-
Window of opportunity for daclizumab.Nat Med. 2011 May;17(5):545-7. doi: 10.1038/nm0511-545. Nat Med. 2011. PMID: 21546970 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
