

Effectiveness of switching from antipsychotic polypharmacy to monotherapy
- PMID: 21536693
- PMCID: PMC3739691
- DOI: 10.1176/appi.ajp.2011.10060908
Effectiveness of switching from antipsychotic polypharmacy to monotherapy
Abstract
Objective: This randomized trial addressed the risks and benefits of staying on antipsychotic polypharmacy or switching to monotherapy.
Method: Adult outpatients with schizophrenia taking two antipsychotics (127 participants across 19 sites) were randomly assigned to stay on polypharmacy or switch to monotherapy by discontinuing one antipsychotic. The trial lasted 6 months, with a 6-month naturalistic follow-up. Kaplan-Meier and Cox regression analyses examined time to discontinuation of assigned antipsychotic treatment, and random regression models examined additional outcomes over time.
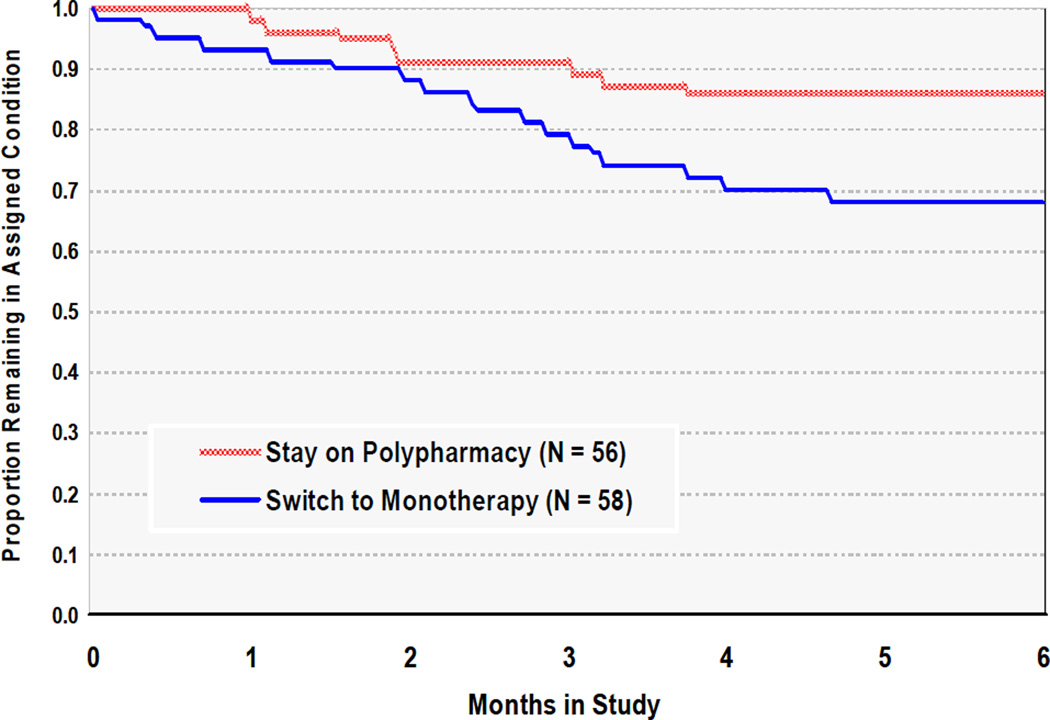
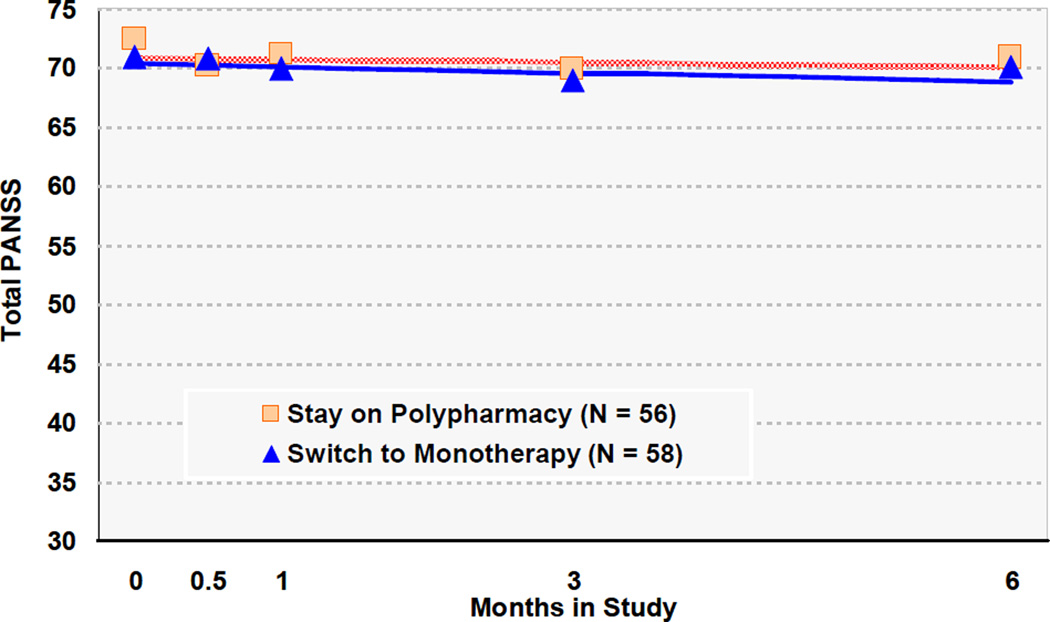
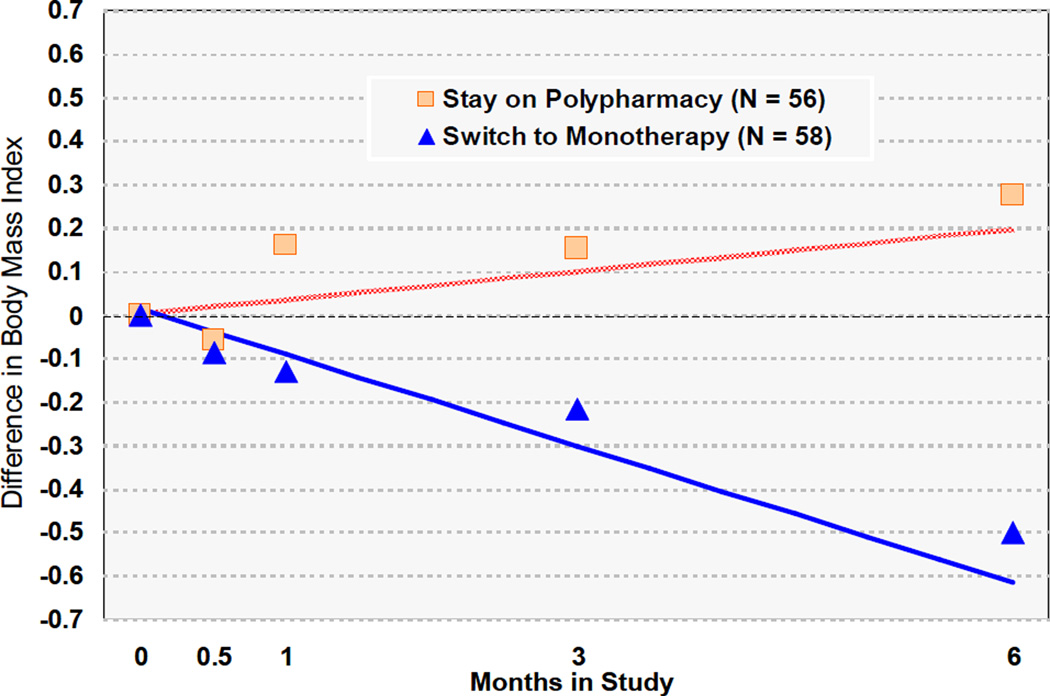
Results: Patients assigned to switch to monotherapy had shorter times to all-cause treatment discontinuation than those assigned to stay on polypharmacy. By month 6, 86% (N=48) of those assigned to stay on polypharmacy were still taking both medications, whereas 69% (N=40) of those assigned to switch to monotherapy were still taking the same medication. Most monotherapy discontinuations entailed returning to the original polypharmacy. The two groups did not differ with respect to psychiatric symptoms or hospitalizations. On average, the monotherapy group lost weight, whereas the polypharmacy group gained weight.
Conclusions: Discontinuing one of two antipsychotics was followed by treatment discontinuation more often and more quickly than when both antipsychotics were continued. However, two-thirds of participants successfully switched, the groups did not differ with respect to symptom control, and switching to monotherapy resulted in weight loss. These results support the reasonableness of prescribing guidelines encouraging trials of antipsychotic monotherapy for individuals receiving antipsychotic polypharmacy, with the caveat that patients should be free to return to polypharmacy if an adequate trial on antipsychotic monotherapy proves unsatisfactory.
Trial registration: ClinicalTrials.gov NCT00044655.
Figures
Comment in
-
Antipsychotic polypharmacy: are two ever better than one?Am J Psychiatry. 2011 Jul;168(7):667-9. doi: 10.1176/appi.ajp.2011.11020314. Am J Psychiatry. 2011. PMID: 21724670 No abstract available.
-
How dosing might influence the conclusion in an antipsychotic polypharmacy effectiveness trial.Am J Psychiatry. 2011 Oct;168(10):1117; author reply 1117. doi: 10.1176/appi.ajp.2011.11050751. Am J Psychiatry. 2011. PMID: 21969048 No abstract available.
References
-
- Essock SM, Covell NH, Leckman-Westin E, Lieberman JA, Sederer L, Kealey E, Finnerty MT members of the Scientific Advisory Committee. Identifying clinically questionable psychotropic prescribing practices for Medicaid recipients in New York State. Psychiatric Services. 2009;60:1595–1602. - PubMed
-
- Tapp A, Wood AE, Secrest L, Erdmann J, Cubberley L, Kilzieh N. Combination Antipsychotic Therapy in Clinical Practice. Psychiatric Services. 2003;54:55–59. - PubMed
-
- Ganguly R, Kotzan JA, Miller LS, Kennedy K, Martin BC. Prevalence, trends, and factors associated with antipsychotic polypharmacy among Medicaid-eligible schizophrenia patients, 1998–2000. J Clin Psychiatry. 2004;65:1377–1388. - PubMed
-
- Centorrino F, Eakin M, Bahk WM, Kelleher JP, Goren J, Salvatore P, Egli S, Baldessarini RJ. Inpatient antipsychotic drug use in 1998, 1993, and 1989. Am J Psychiatry. 2002;159:1932–1935. - PubMed
-
- Clark RE, Bartels SJ, Mellman TA, Peacock WJ. Recent trends in antipsychotic combination therapy of schizophrenia and schizoaffective disorder: implications for state mental health policy. Schizophr Bull. 2002;28:75–84. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
