

X-ray magnetic resonance fusion to internal markers and utility in congenital heart disease catheterization
- PMID: 21536785
- PMCID: PMC3568502
- DOI: 10.1161/CIRCIMAGING.111.963868
X-ray magnetic resonance fusion to internal markers and utility in congenital heart disease catheterization
Abstract
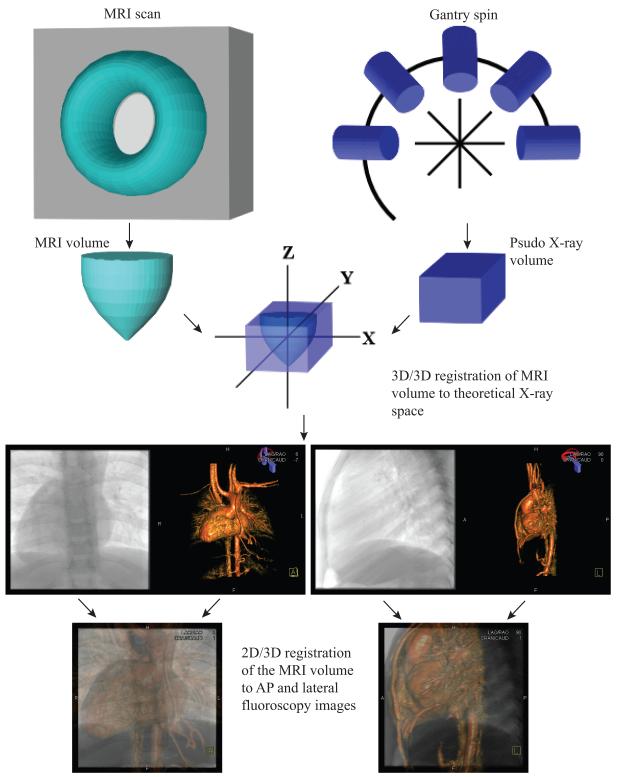
Background: X-ray magnetic resonance fusion (XMRF) allows for use of 3D data during cardiac catheterization. However, to date, technical requirements have limited the use of this modality in clinical practice. We report on a new internal-marker XMRF method that we have developed and describe how we used XMRF during cardiac catheterization in congenital heart disease.
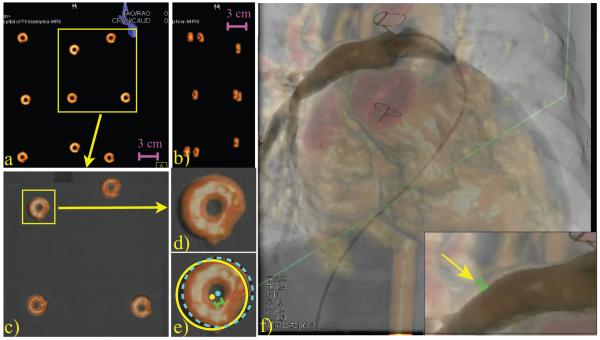
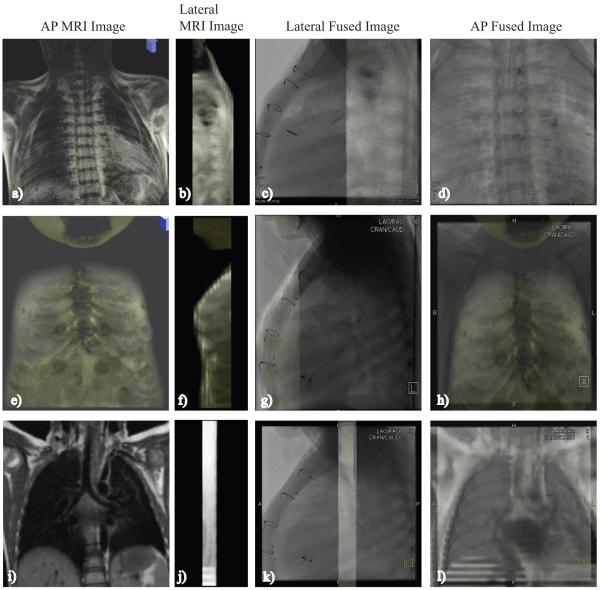
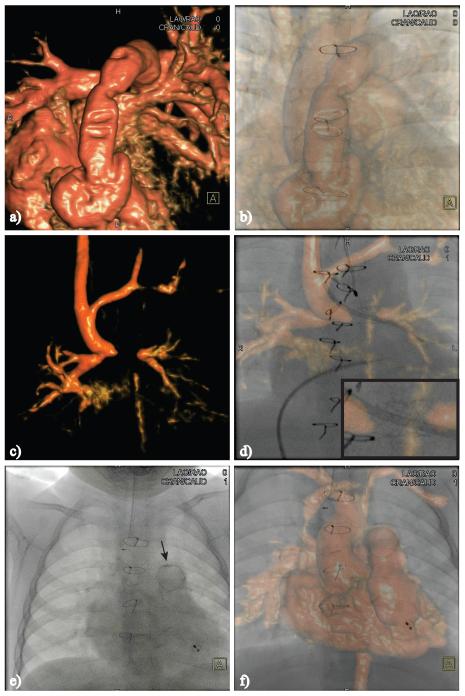
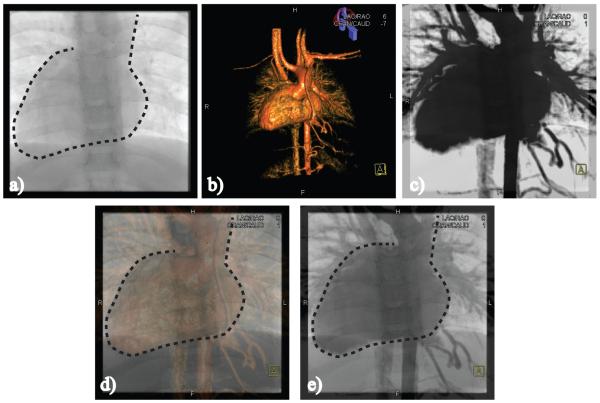
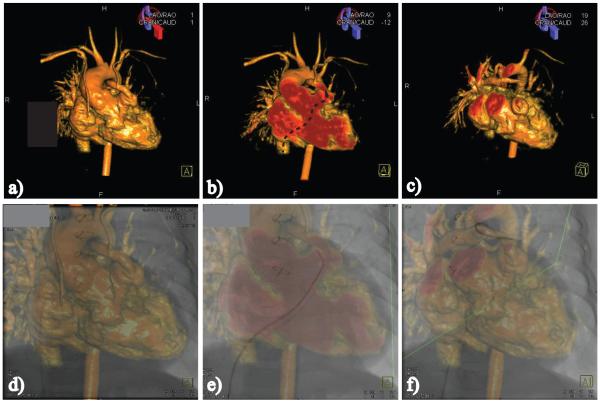
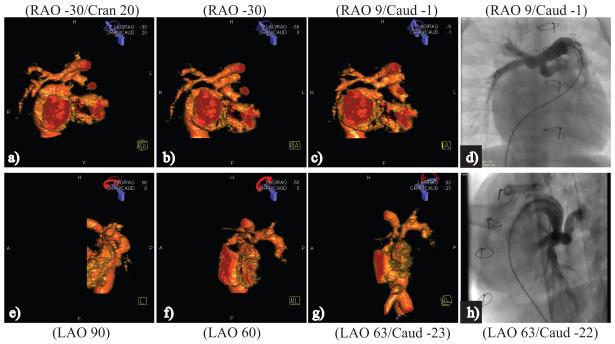
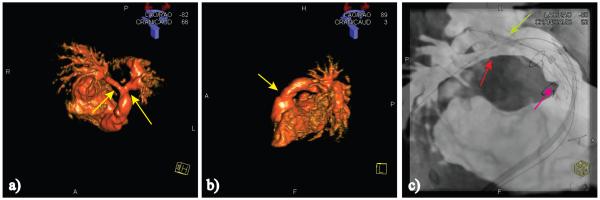
Methods and results: XMRF was performed in a phantom and in 23 patients presenting for cardiac catheterization who also needed cardiac MRI for clinical reasons. The registration process was performed in < 5 minutes per patient, with minimal radiation (0.004 to 0.024 mSv) and without contrast. Registration error was calculated in a phantom and in 8 patients using the maximum distance between angiographic and 3D model boundaries. In the phantom, the measured error in the anteroposterior projection had a mean of 1.15 mm (standard deviation, 0.73). The measured error in patients had a median of 2.15 mm (interquartile range, 1.65 to 2.56 mm). Internal markers included bones, airway, image artifact, calcifications, and the heart and vessel borders. The MRI data were used for road mapping in 17 of 23 (74%) cases and camera angle selection in 11 of 23 (48%) cases.
Conclusions: Internal marker-based registration can be performed quickly, with minimal radiation, without the need for contrast, and with clinically acceptable accuracy using commercially available software. We have also demonstrated several potential uses for XMRF in routine clinical practice. This modality has the potential to reduce radiation exposure and improve catheterization outcomes.
Figures
Comment in
-
Roadmaps show the way: coregistration to enhance structural heart interventions.Catheter Cardiovasc Interv. 2013 Sep 1;82(3):443-4. doi: 10.1002/ccd.25115. Catheter Cardiovasc Interv. 2013. PMID: 24038978 Free PMC article. No abstract available.
References
-
- Knecht S, Skali H, O’Neill MD, Wright M, Matsuo S, Chaudhry GM, Haffajee CI, Nault I, Gijsbers GH, Sacher F, Laurent F, Montaudon M, Corneloup O, Hocini M, Haissaguerre M, Orlov MV, Jais P. Computed tomography-fluoroscopy overlay evaluation during catheter ablation of left atrial arrhythmia. Europace. 2008;10:931–938. - PubMed
-
- Sra J, Krum D, Malloy A, Vass M, Belanger B, Soubelet E, Vaillant R, Akhtar M. Registration of three-dimensional left atrial computed tomographic images with projection images obtained using fluoroscopy. Circulation. 2005;112:3763–3768. - PubMed
-
- Sra J, Narayan G, Krum D, Akhtar M. Registration of 3d computed tomographic images with interventional systems: implications for catheter ablation of atrial fibrillation. J Interv Card Electrophysiol. 2006;16:141–148. - PubMed
-
- Sra J, Narayan G, Krum D, Malloy A, Cooley R, Bhatia A, Dhala A, Blanck Z, Nangia V, Akhtar M. Computed tomography-fluoroscopy image integration-guided catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 2007;18:409–414. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
