

Identifying patients harboring extended-spectrum-beta-lactamase-producing Enterobacteriaceae on hospital admission: derivation and validation of a scoring system
- PMID: 21537020
- PMCID: PMC3122446
- DOI: 10.1128/AAC.00009-11
Identifying patients harboring extended-spectrum-beta-lactamase-producing Enterobacteriaceae on hospital admission: derivation and validation of a scoring system
Abstract
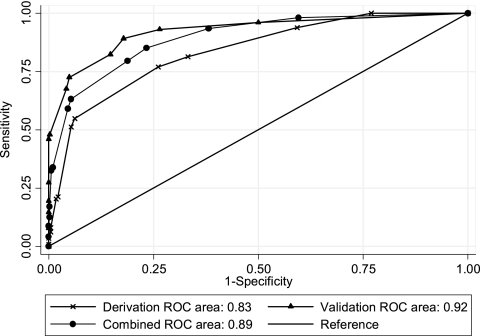
Increases in community-acquired infections caused by extended-spectrum-β-lactamase (ESBL)-producing Enterobacteriaceae have important implications for hospital infection control and empirical antibiotic therapy protocols. We developed and validated a tool for identifying patients harboring these organisms at hospital admission. We retrospectively analyzed chart data for 849 adult inpatients. The derivation cohort included 339 patients admitted to a large hospital in Rome during 2008, with (n = 113) or without (n = 226) culture positivity for ESBL-producing Escherichia coli, Klebsiella spp., or Proteus mirabilis within 48 h after admission. Logistic-regression-based prediction scores were calculated based on variables independently associated with the outcome. The model was validated in a second cohort (n = 510) selected with identical criteria in hospitals in Genoa and Turin during 2009. Prediction scores were based on the following six variables (reported with odds ratio for study outcome and the 95% confidence intervals in brackets): recent (≤ 12 months before admission) hospitalization (5.69 [2.94 to 10.99]), transfer from another health care facility (5.61 [1.65 to 19.08]), Charlson comorbidity score ≥ 4 (3.80 [1.90 to 7.59]), recent (≤ 3 months before admission) β-lactam and/or fluoroquinolone treatment (3.68 [1.96 to 6.91]), recent urinary catheterization (3.52 [1.96 to 6.91]), and age ≥ 70 years (3.20 [1.79 to 5.70]). The model displayed good calibration and good-to-excellent discrimination in the derivation and validation sets (Hosmer-Lemshow χ(2) = 15.28 and 14.07; P = 0.17 and 0.23; areas under the receiver-operating characteristic curve, 0.83 and 0.92). It reliably identified patients likely to be harboring ESBL-producing Enterobacteriaceae at hospital admission who may need special infection control measures. Further study is needed to confirm this model's potential as a guide for prescribing empirical antibiotic therapy.
Figures
Comment in
-
Identifying patients harboring extended-spectrum-β-lactamase-producing Enterobacteriaceae on hospital admission is not that simple.Antimicrob Agents Chemother. 2012 Apr;56(4):2218-9; author reply 2220. doi: 10.1128/AAC.06376-11. Antimicrob Agents Chemother. 2012. PMID: 22427458 Free PMC article. No abstract available.
References
-
- Apisarnthanarak A., Kiratisin P., Mundy L. M. 2008. Predictors of mortality from community-onset bloodstream infections due to extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae. Infect. Control Hosp. Epidemiol. 29:671–674 - PubMed
-
- Azap O. K., et al. 2010. Risk factors for extended-spectrum beta-lactamase positivity in uropathogenic Escherichia coli isolated from community-acquired urinary tract infections. Clin. Microbiol. Infect. 16:147–151 - PubMed
-
- Ben-Ami R., et al. 2009. A multinational survey of risk factors for infection with extended-spectrum beta-lactamase-producing enterobacteriaceae in nonhospitalized patients. Clin. Infect. Dis. 49:682–690 - PubMed
-
- Ben-Ami R., et al. 2006. Influx of extended-spectrum beta-lactamase-producing Enterobacteriaceae into the hospital. Clin. Infect. Dis. 42:925–934 - PubMed
-
- Charlson M. E., Pompei P., Ales K. L., MacKenzie C. R. 1987. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40:373–383 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
