

Fever screening during the influenza (H1N1-2009) pandemic at Narita International Airport, Japan
- PMID: 21539735
- PMCID: PMC3096599
- DOI: 10.1186/1471-2334-11-111
Fever screening during the influenza (H1N1-2009) pandemic at Narita International Airport, Japan
Abstract
Background: Entry screening tends to start with a search for febrile international passengers, and infrared thermoscanners have been employed for fever screening in Japan. We aimed to retrospectively assess the feasibility of detecting influenza cases based on fever screening as a sole measure.
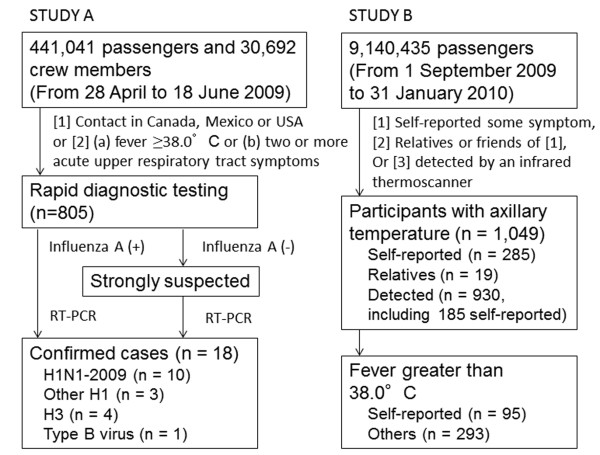
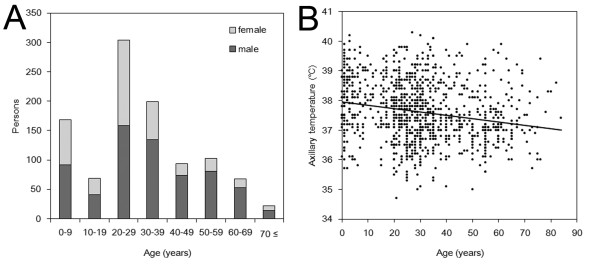
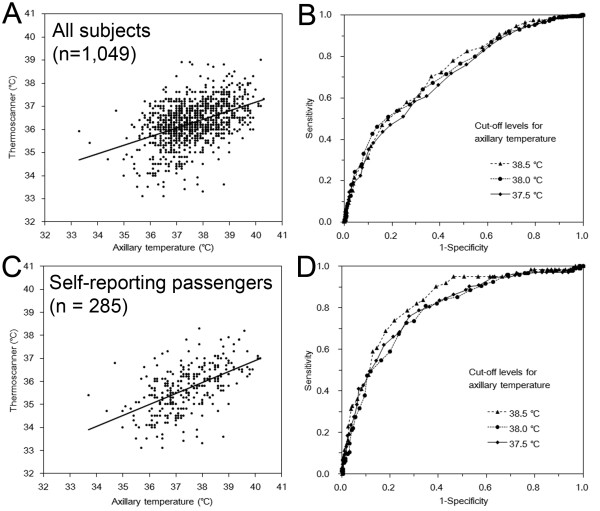
Methods: Two datasets were collected at Narita International Airport during the 2009 pandemic. The first contained confirmed influenza cases (n = 16) whose diagnosis took place at the airport during the early stages of the pandemic, and the second contained a selected and suspected fraction of passengers (self-reported or detected by an infrared thermoscanner; n = 1,049) screened from September 2009 to January 2010. The sensitivity of fever (38.0 °C) for detecting H1N1-2009 was estimated, and the diagnostic performances of the infrared thermoscanners in detecting hyperthermia at cut-off levels of 37.5 °C, 38.0 °C and 38.5 °C were also estimated.
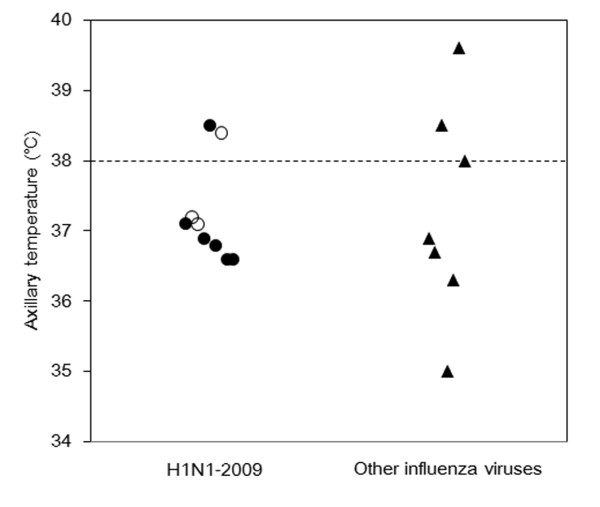
Results: The sensitivity of fever for detecting H1N1-2009 cases upon arrival was estimated to be 22.2% (95% confidence interval: 0, 55.6) among nine confirmed H1N1-2009 cases, and 55.6% of the H1N1-2009 cases were under antipyretic medications upon arrival. The sensitivity and specificity of the infrared thermoscanners in detecting hyperthermia ranged from 50.8-70.4% and 63.6-81.7%, respectively. The positive predictive value appeared to be as low as 37.3-68.0%.
Conclusions: The sensitivity of entry screening is a product of the sensitivity of fever for detecting influenza cases and the sensitivity of the infrared thermoscanners in detecting fever. Given the additional presence of confounding factors and unrestricted medications among passengers, reliance on fever alone is unlikely to be feasible as an entry screening measure.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
