

Incomplete recovery of myocyte contractile function despite improvement of myocardial architecture with left ventricular assist device support
- PMID: 21540356
- PMCID: PMC3407673
- DOI: 10.1161/CIRCHEARTFAILURE.111.961326
Incomplete recovery of myocyte contractile function despite improvement of myocardial architecture with left ventricular assist device support
Abstract
Background: Unloading a failing heart with a left ventricular assist device (LVAD) can improve ejection fraction (EF) and LV size; however, recovery with LVAD explantation is rare. We hypothesized that evaluation of myocyte contractility and biochemistry at the sarcomere level before and after LVAD may explain organ-level changes.
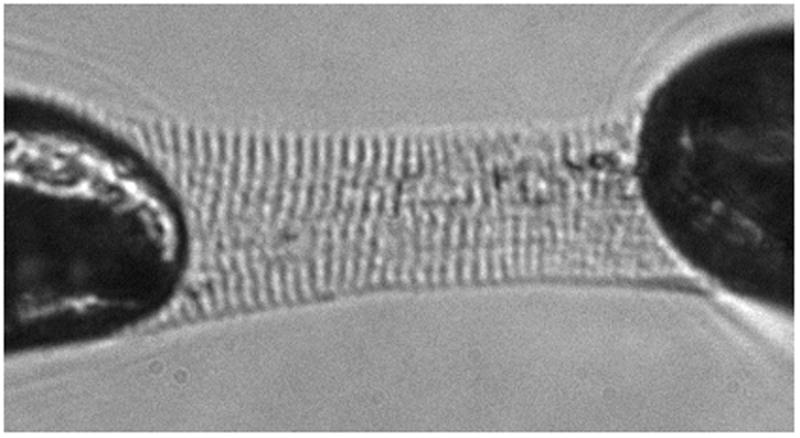
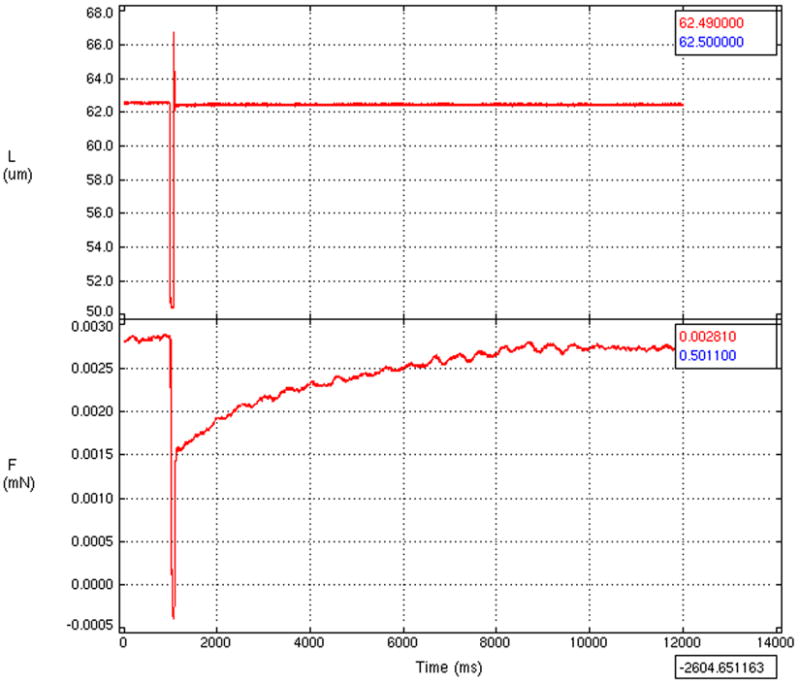
Methods and results: Paired LV tissue samples were frozen from 8 patients with nonischemic cardiomyopathy at LVAD implantation (before LVAD) and before cardiac transplantation (after LVAD). These were compared with 8 nonfailing hearts. Isolated skinned myocytes were purified and attached to a force transducer, and dimensions, maximum calcium-saturated force, calcium sensitivity, and myofilament cooperativity were assessed. Relative isoform abundance and phosphorylation levels of sarcomeric contractile proteins were measured. With LVAD support, the unloaded EF improved (10.0±1.0% to 25.6±11.0%, P=0.007), LV size decreased (LV internal dimension at end diastole, 7.6±1.2 to 4.9±1.4 cm; P<0.001), and myocyte dimensions decreased (cross-sectional area, 1247±346 to 638±254 μm(2); P=0.001). Maximum calcium-saturated force improved after LVAD (3.6±0.9 to 7.3±1.8 mN/mm(2), P<0.001) implantation but was still lower than in nonfailing hearts (7.3±1.8 versus 17.6±1.8 mN/mm(2), P<0.001). An increase in troponin I (TnI) phosphorylation after LVAD implantation was noted, but protein kinase C phosphorylation of TnI decreased. Biochemical changes of other sarcomeric proteins were not observed after LVAD.
Conclusions: There is significant improvement in LV and myocyte size with LVAD, but there is only partial recovery of EF and myocyte contractility. LVAD support was associated only with biochemical changes in TnI, suggesting that alternate mechanisms might contribute to contractile changes after LVAD and that additional interventions may be needed to alter biochemical remodeling of the sarcomere to further enhance myofilament and organ-level recovery.
Figures




Comment in
-
Bridge to recovery and the search for decision nodes.Circ Heart Fail. 2011 Jul;4(4):393-5. doi: 10.1161/CIRCHEARTFAILURE.111.963058. Circ Heart Fail. 2011. PMID: 21772015 No abstract available.
References
-
- Maybaum S, Mancini D, Xydas S, Starling RC, Aaronson K, Pagani FD, Miller LW, Margulies K, McRee S, Frazier OH, Torre-Amione G. Cardiac improvement during mechanical circulatory support: A prospective multicenter study of the LVAD working group. Circulation. 2007;115:2497–2505. - PubMed
-
- Burkhoff D, Klotz S, Mancini DM. LVAD-induced reverse remodeling: Basic and clinical implications for myocardial recovery. J of Card Failure. 2006;12:227–239. - PubMed
-
- Bruggink AH, de Jonge N, van Oosterhout MF, Van Wichen DF, de Koning E, Lahpor JR, Kemperman H, Gmelig-Meyling FH, de Weger RA. Brain natriuretic peptide is produced both by cardiomyocytes and cells infiltrating the heart in patients with severe heart failure supported by a left ventricular assist device. J Heart Lung Transplant. 2006;25:174–180. - PubMed
-
- Torre-Amione G, Stetson SJ, Youker KA, Durand JB, Radovancevic B, Delgado RM, Frazier OH, Entman ML, Noon GP. Decreased expression of tumor necrosis factor-α in failing human myocardium after mechanical circulatory support: A potential mechanism for cardiac recovery. Circulation. 1999;100:1189–1193. - PubMed
-
- Zafeiridis A, Jeevanandam V, Houser SR, Margulies KB. Regression of cellular hypertrophy after left ventricular assist device support. Circulation. 1998;98:656–662. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
