

Risk factors for non-adherence and loss to follow-up in a three-year clinical trial in Botswana
- PMID: 21541021
- PMCID: PMC3081815
- DOI: 10.1371/journal.pone.0018435
Risk factors for non-adherence and loss to follow-up in a three-year clinical trial in Botswana
Abstract
Background: Participant non-adherence and loss to follow-up can compromise the validity of clinical trial results. An assessment of these issues was made in a 3-year tuberculosis prevention trial among HIV-infected adults in Botswana.
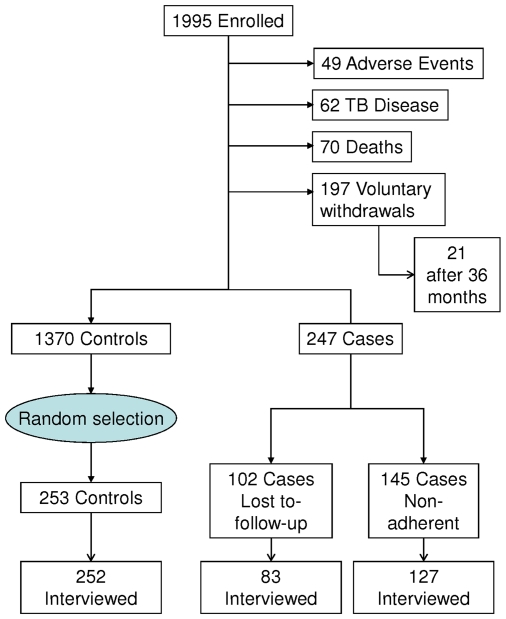
Methods and findings: Between 11/2004-07/2006, 1995 participants were enrolled at eight public health clinics. They returned monthly to receive bottles of medication and were expected to take daily tablets of isoniazid or placebo for three years. Non-adherence was defined as refusing tablet ingestion but agreeing to quarterly physical examinations. Loss to follow-up was defined as not having returned for appointments in ≥60 days. Between 10/2008-04/2009, survey interviews were conducted with 83 participants identified as lost to follow-up and 127 identified as non-adherent. As a comparison, 252 randomly selected adherent participants were also surveyed. Multivariate logistic regression analysis was used to identify associations with selected risk factors. Men had higher odds of being non-adherent (adjusted odds ratio (AOR), 2.24; 95% confidence interval [95%CI] 1.24-4.04) and lost to follow-up (AOR 3.08; 95%CI 1.50-6.33). Non-adherent participants had higher odds of reporting difficulties taking the regimen or not knowing if they had difficulties (AOR 3.40; 95%CI 1.75-6.60) and lower odds associated with each year of age (AOR 0.95; 95%CI 0.91-0.98), but other variables such as employment, distance from clinic, alcohol use, and understanding study requirements were not significantly different than controls. Among participants who were non-adherent or lost to follow-up, 40/210 (19.0%) reported that they stopped the medication because of work commitments and 33/210 (15.7%) said they thought they had completed the study.
Conclusions: Men had higher odds of non-adherence and loss to follow-up than women. Potential interventions that might improve adherence in trial participants may include:targeting health education for men, reducing barriers, clarifying study expectations, educating employers about HIV/AIDS to help reduce stigma in the workplace, and encouraging employers to support employee health.
Trial registration: ClinicalTrials.gov NCT00164281.
Conflict of interest statement
Figures
References
-
- Samandari T, Agizew T, Nyirenda S, Tedla Z, Sibanda T, et al. 6-month versus 36-month isoniazid preventive treatment for tuberculosis in adults with HIV-infection in Botswana:a randomized, double-blind, placebo-controlled trial. Lancet. 2011 in press. - PubMed
-
- Bucher HC, Griffith LE, Guyatt GH, Sudre P, Naef M, et al. Isoniazid prophylaxis for tuberculosis in HIV infection:a meta-analysis of randomized controlled trials. AIDS. 1999;13:501–7. - PubMed
-
- Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487–97. - PubMed
-
- Ngamvithayapong J, Uthaivoravit W, Yanai H, Akarasewi P, Sawanpanyalert P. Adherence to tuberculosis preventive therapy among HIV-infected persons in Chiang Rai, Thailand. AIDS. 1997;11:107–12. - PubMed
-
- Amico KR, Harman JJ, O'Grady MA. Attrition and related trends in scientific rigor:a score card for ART adherence intervention research and recommendations for future directions. Curr HIV /AIDS Rep. 2008;5:172–85. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
