

Discrepancies between prescribed and defined daily doses: a matter of patients or drug classes?
- PMID: 21544512
- PMCID: PMC3134712
- DOI: 10.1007/s00228-011-1014-7
Discrepancies between prescribed and defined daily doses: a matter of patients or drug classes?
Abstract
Purpose: Defined daily doses (DDD) are used for the measurement of drug utilisation. The aim of the study was to analyse whether differences between DDD and prescribed daily doses (PDD) exist for relevant drug classes such as antihypertensive drugs and, if so, whether they primarily depend on drug classes or patient-related factors.
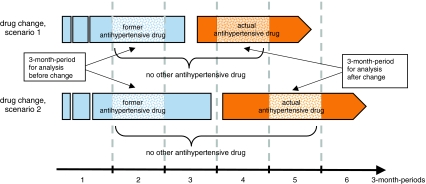
Methods: Using the data of a large German statutory health insurance scheme, we analysed continuous prescriptions for the following antihypertensive drug classes: thiazide diuretics, beta-blockers, dihydropyridine calcium channel blockers (CCBs), angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin-II receptor blockers (ARBs). We summed the doses of all dispensed drugs per person during a defined time frame. We calculated the PDD (= total dose divided by the number of days) and expressed them as the PDD:DDD ratio (= amount of DDD per day and person).
Results: During the study period, 149,704 patients continuously received an antihypertensive medication. The average PDD:DDD ratio ranged from 0.84 (beta-blockers) to 1.88 (ARBs) and 2.17 (ACEIs). The average prescribed dosage of each drug class remained unchanged, even if the patients had previously received another antihypertensive drug with another PDD:DDD ratio. For example, if patients were switched from a beta-blocker to an ACEI, the PDD:DDD ratio increased, on average, from 0.79 to 2.17. Vice versa, the ratio decreased for patients with a drug change from an ACEI to a beta-blocker from 2.06 to 0.75.
Conclusions: Even large differences between DDD and PDD seem to be a matter of drug classes and not primarily of patient characteristics.
References
-
- WHO Collaborating Centre for Drug Statistics Methodology (2009) Guidelines for ATC classification and DDD assignment 2010. http://www.whocc.no/filearchive/publications/2010guidelines.pdf. Accessed 5 January 2011
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
