

The interaction of respiration and visual feedback on the control of force and neural activation of the agonist muscle
- PMID: 21546109
- PMCID: PMC3202062
- DOI: 10.1016/j.humov.2010.09.007
The interaction of respiration and visual feedback on the control of force and neural activation of the agonist muscle
Abstract
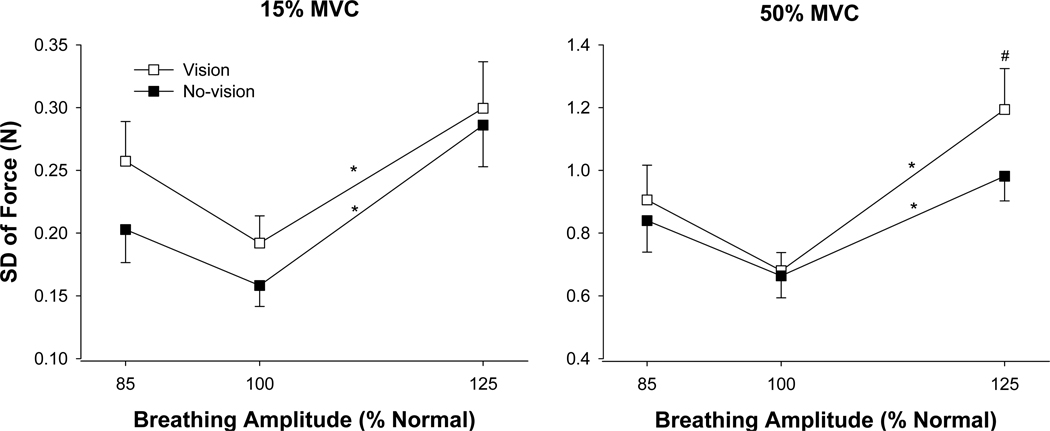
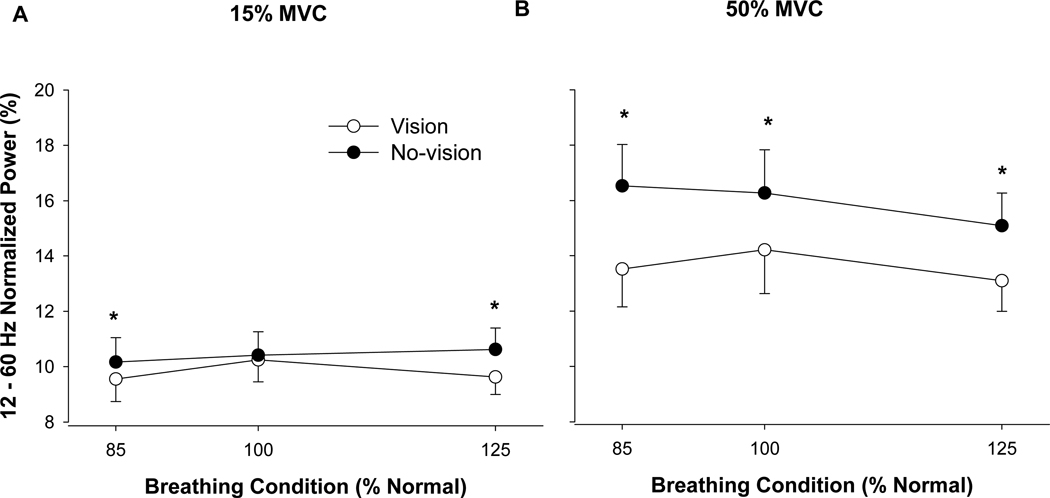
The purpose of this study was to compare force variability and the neural activation of the agonist muscle during constant isometric contractions at different force levels when the amplitude of respiration and visual feedback were varied. Twenty young adults (20-32 years, 10 men and 10 women) were instructed to accurately match a target force at 15% and 50% of their maximal voluntary contraction (MVC) with abduction of the index finger while controlling their respiration at different amplitudes (85%, 100% and 125% normal) in the presence and absence of visual feedback. Each trial lasted 22s and visual feedback was removed from 8-12 and 16-20s. Each subject performed three trials with each respiratory condition at each force level. Force variability was quantified as the standard deviation of the detrended force data. The neural activation of the first dorsal interosseus (FDI) was measured with bipolar surface electrodes placed distal to the innervation zone. Relative to normal respiration, force variability increased significantly only during high-amplitude respiration (∼63%). The increase in force variability from normal- to high-amplitude respiration was strongly associated with amplified force oscillations from 0 to 3 Hz (R(2) ranged from .68 to .84, p< .001). Furthermore, the increase in force variability was exacerbated in the presence of visual feedback at 50% MVC (vision vs. no-vision: .97 vs. .87N) and was strongly associated with amplified force oscillations from 0 to 1 Hz (R(2)= .82) and weakly associated with greater power from 12 to 30 Hz (R(2)= .24) in the EMG of the agonist muscle. Our findings demonstrate that high-amplitude respiration and visual feedback of force interact and amplify force variability in young adults during moderate levels of effort.
Copyright © 2011 Elsevier B.V. All rights reserved.
Figures





References
-
- Addison PS. The illustrated wavelet transform handbook. New York: Taylor & Francis Group, New York; 2002.
-
- Brown P. Cortical drives to human muscle: The Piper and related rhythms. Progress in Neurobiology. 2000;60:97–108. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
