

CT cerebral blood flow maps optimally correlate with admission diffusion-weighted imaging in acute stroke but thresholds vary by postprocessing platform
- PMID: 21546490
- PMCID: PMC3125441
- DOI: 10.1161/STROKEAHA.110.610618
CT cerebral blood flow maps optimally correlate with admission diffusion-weighted imaging in acute stroke but thresholds vary by postprocessing platform
Abstract
Background and purpose: Admission infarct core lesion size is an important determinant of management and outcome in acute (<9 hours) stroke. Our purposes were to: (1) determine the optimal CT perfusion parameter to define infarct core using various postprocessing platforms; and (2) establish the degree of variability in threshold values between these different platforms.
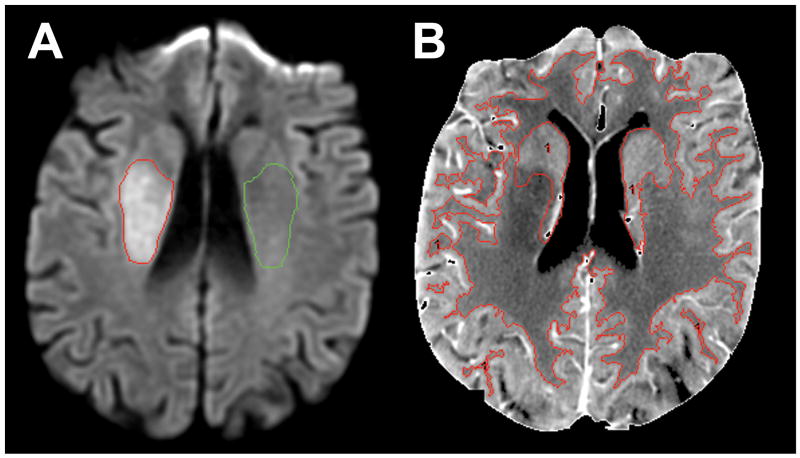
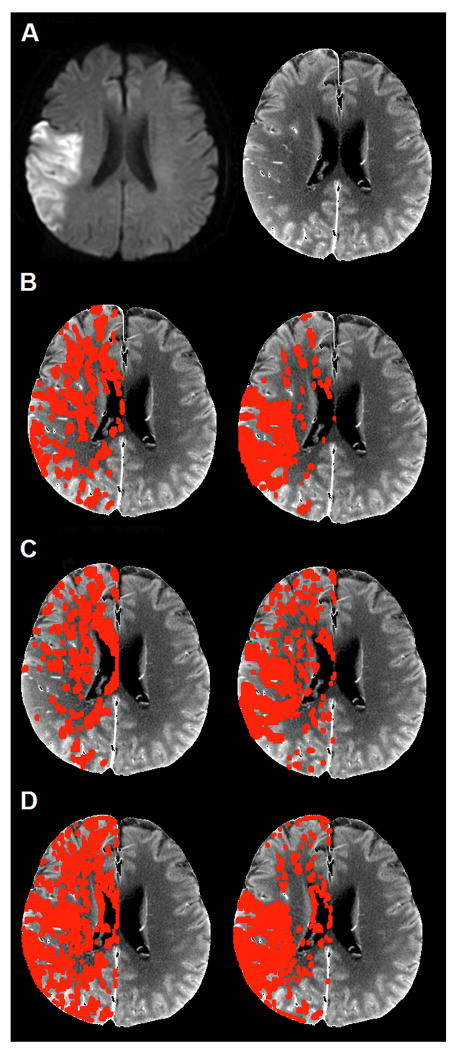
Methods: We evaluated 48 consecutive cases with vessel occlusion and admission CT perfusion and diffusion-weighted imaging within 3 hours of each other. CT perfusion was acquired with a "second-generation" 66-second biphasic cine protocol and postprocessed using "standard" (from 2 vendors, "A-std" and "B-std") and "delay-corrected" (from 1 vendor, "A-dc") commercial software. Receiver operating characteristic curve analysis was performed comparing each CT perfusion parameter-both absolute and normalized to the contralateral uninvolved hemisphere-between infarcted and noninfarcted regions as defined by coregistered diffusion-weighted imaging.
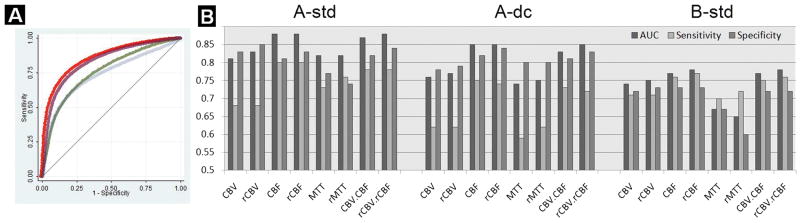
Results: Cerebral blood flow had the highest accuracy (receiver operating characteristic area under the curve) for all 3 platforms (P<0.01). The maximal areas under the curve for each parameter were: absolute cerebral blood flow 0.88, cerebral blood volume 0.81, and mean transit time 0.82 and relative Cerebral blood flow 0.88, cerebral blood volume 0.83, and mean transit time 0.82. Optimal receiver operating characteristic operating point thresholds varied significantly between different platforms (Friedman test, P<0.01).
Conclusions: Admission absolute and normalized "second-generation" cine acquired CT cerebral blood flow lesion volumes correlate more closely with diffusion-weighted imaging-defined infarct core than do those of CT cerebral blood volume or mean transit time. Although limited availability of diffusion-weighted imaging for some patients creates impetus to develop alternative methods of estimating core, the marked variability in quantification among different postprocessing software limits generalizability of parameter map thresholds between platforms.
Figures
References
-
- Hacke W, Kaste M, Fieschi C, Toni D, Lesaffre E, von Kummer R, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS) JAMA. 1995;274:1017–1025. - PubMed
-
- Ueda T, Sakaki S, Yuh WT, Nochide I, Ohta S. Outcome in acute stroke with successful intra-arterial thrombolysis and predictive value of initial single-photon emission-computed tomography. J Cereb Blood Flow Metab. 1999;19:99–108. - PubMed
-
- Schellinger PD, Bryan RN, Caplan LR, Detre JA, Edelman RR, Jaigobin C, et al. Evidence-based guideline: The role of diffusion and perfusion MRI for the diagnosis of acute ischemic stroke: Report of the therapeutics and technology assessment subcommittee of the american academy of neurology. Neurology. 2010;75:177–185. - PMC - PubMed
-
- Lev MH, Farkas J, Gemmete JJ, Hossain ST, Hunter GJ, Koroshetz WJ, et al. Acute stroke: Improved nonenhanced CT detection--benefits of soft-copy interpretation by using variable window width and center level settings. Radiology. 1999;213:150–155. - PubMed
-
- Shetty SK, Lev MH. CT perfusion in acute stroke. Neuroimaging Clin N Am. 2005;15:481–501. ix. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
