

Clinicopathological and prognostic implications of genetic alterations in oral cancers
- PMID: 21546976
- PMCID: PMC3085881
- DOI: 10.3892/ol.2011.271
Clinicopathological and prognostic implications of genetic alterations in oral cancers
Abstract
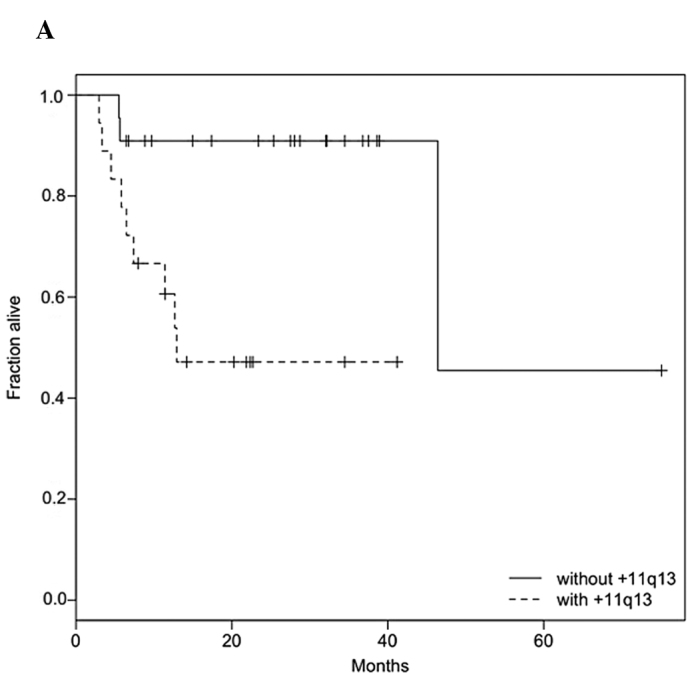
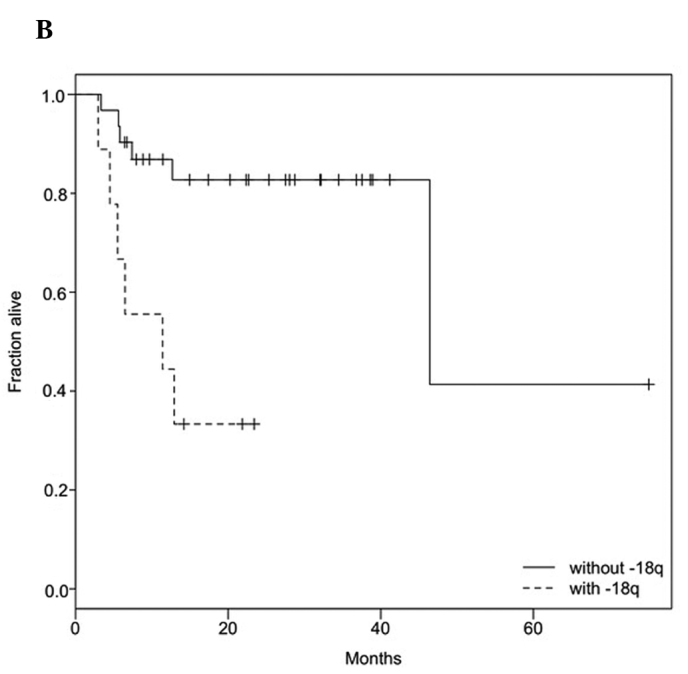
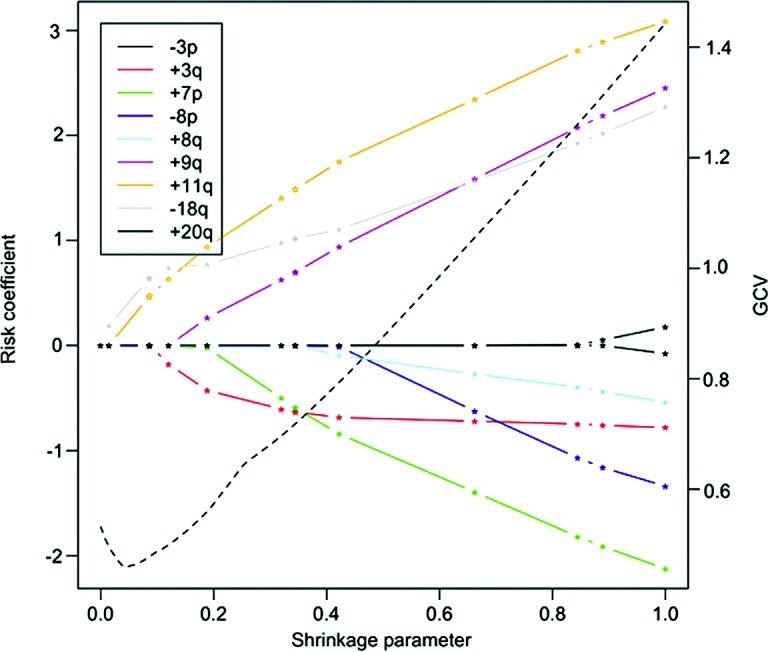
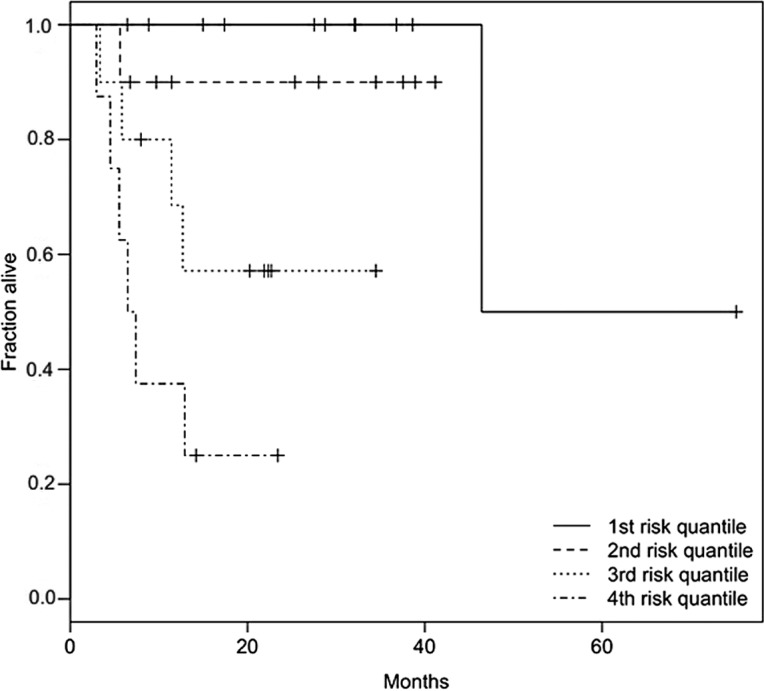
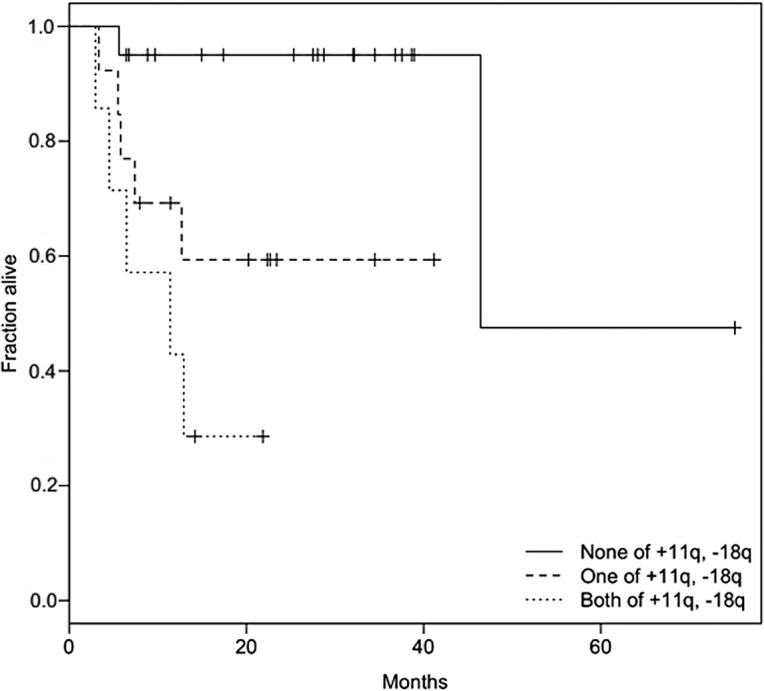
This study evaluated the clinicopathological and prognostic implications of genetic alterations characterizing oral squamous cell carcinoma(OSCC). Comparative genomic hybridization(CGH) was used to identify chromosomal alterations present in primary OSCCs obtained from 97 pateints. In this population, tobacco use was a significant risk factor for OSCC. By contrast, all 97 of our samples are negative for human papillomavirus (HPV) DNA integration, which is another known risk factor for OSCC in certain populations. Results of the Fisher's exact test followed by Benjamini-Hochberg correction for multiple testing, showed a correlation of 7p gain and 8p loss with node-positive OSCC (p≤0.04 for both genetic alterations) and association of 11q13 gain with high-grade OSCC (p≤0.05). Univariate Cox-proportional hazard models, also corrected for multiple testing, showed significant association of 11q13 gain and 18q loss with decreased survival (p≤0.05). These findings were supported by multivariate analysis which revealed that 11q13 gain and 18q loss together serve as a strong bivariate predictor of poor prognosis. In conclusion, our study has identified genetic alterations that correlate significantly with nodal status, grade, and poor survival status of OSCC. These potential biomarkers may aid the current TNM system for better prediction of clinical outcome.
Figures
Similar articles
-
Genetic signatures of HPV-related and unrelated oropharyngeal carcinoma and their prognostic implications.Clin Cancer Res. 2009 Mar 1;15(5):1779-86. doi: 10.1158/1078-0432.CCR-08-1463. Epub 2009 Feb 17. Clin Cancer Res. 2009. PMID: 19223504
-
Genome wide profiling in oral squamous cell carcinoma identifies a four genetic marker signature of prognostic significance.PLoS One. 2017 Apr 6;12(4):e0174865. doi: 10.1371/journal.pone.0174865. eCollection 2017. PLoS One. 2017. PMID: 28384287 Free PMC article.
-
Loss of 3p26.3 is an independent prognostic factor in patients with oral squamous cell carcinoma.Oncol Rep. 2011 Aug;26(2):463-9. doi: 10.3892/or.2011.1327. Epub 2011 May 26. Oncol Rep. 2011. PMID: 21617881
-
Chromosomal imbalances in oral squamous cell carcinoma: examination of 31 cell lines and review of the literature.Oral Oncol. 2008 Apr;44(4):369-82. doi: 10.1016/j.oraloncology.2007.05.003. Epub 2007 Aug 2. Oral Oncol. 2008. PMID: 17681875 Free PMC article. Review.
-
Relationship of programmed death ligand-1 expression with clinicopathological features and prognosis in patients with oral squamous cell carcinoma: A meta-analysis.Arch Oral Biol. 2020 Jun;114:104717. doi: 10.1016/j.archoralbio.2020.104717. Epub 2020 Apr 11. Arch Oral Biol. 2020. PMID: 32344357 Review.
Cited by
-
Genomic profiling of oral squamous cell carcinoma by array-based comparative genomic hybridization.PLoS One. 2013;8(2):e56165. doi: 10.1371/journal.pone.0056165. Epub 2013 Feb 14. PLoS One. 2013. PMID: 23457519 Free PMC article.
-
(Cyto)genomic and epigenetic characterization of BICR 10 cell line and three new established primary human head and neck squamous cell carcinoma cultures.Genes Genomics. 2019 Oct;41(10):1207-1221. doi: 10.1007/s13258-019-00850-6. Epub 2019 Jul 18. Genes Genomics. 2019. PMID: 31321735
-
Clinical relevance of copy number profiling in oral and oropharyngeal squamous cell carcinoma.Cancer Med. 2015 Oct;4(10):1525-35. doi: 10.1002/cam4.499. Epub 2015 Jul 21. Cancer Med. 2015. PMID: 26194878 Free PMC article.
-
Clinico-Pathological Correlation of β-Catenin and Telomere Dysfunction in Head and Neck Squamous Cell Carcinoma Patients.J Cancer. 2015 Jan 15;6(2):192-202. doi: 10.7150/jca.9558. eCollection 2015. J Cancer. 2015. PMID: 25653721 Free PMC article.
-
Notch pathway activation is essential for maintenance of stem-like cells in early tongue cancer.Oncotarget. 2016 Aug 2;7(31):50437-50449. doi: 10.18632/oncotarget.10419. Oncotarget. 2016. PMID: 27391340 Free PMC article.
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Notani P. Epidemiology and prevention of head and neck cancer: a global view. In: Saranath D, editor. Contemporary Issues in Oral Cancer. Oxford University Press; New Delhi: 2000. pp. 1–29.
-
- Nair U, Bartsch H, Nair J. Alert for an epidemic of oral cancer due to use of the betel quid substitutes gutkha and pan masala: a review of agents and causative mechanisms. Mutagenesis. 2004;19:251–262. - PubMed
-
- Akervall J. Genomic screening of head and neck cancer and its implications for therapy planning. Eur Arch Otorhinolaryngol. 2006;263:297–304. - PubMed
-
- Hermsen M, Joenje H, Arwert F, et al. Assessment of chromosomal gains and losses in oral squamous cell carcinoma by comparative genomic hybridisation. Oral Oncol. 1997;33:414–418. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources