

Review of osteoimmunology and the host response in endodontic and periodontal lesions
- PMID: 21547019
- PMCID: PMC3087239
- DOI: 10.3402/jom.v3i0.5304
Review of osteoimmunology and the host response in endodontic and periodontal lesions
Abstract
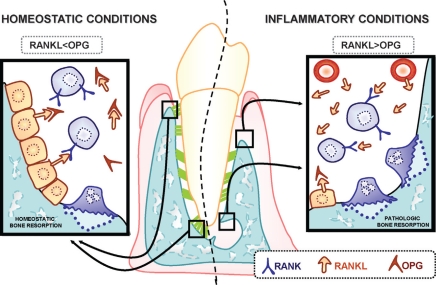
Both lesions of endodontic origin and periodontal diseases involve the host response to bacteria and the formation of osteolytic lesions. Important for both is the upregulation of inflammatory cytokines that initiate and sustain the inflammatory response. Also important are chemokines that induce recruitment of leukocyte subsets and bone-resorptive factors that are largely produced by recruited inflammatory cells. However, there are differences also. Lesions of endodontic origin pose a particular challenge since that bacteria persist in a protected reservoir that is not readily accessible to the immune defenses. Thus, experiments in which the host response is inhibited in endodontic lesions tend to aggravate the formation of osteolytic lesions. In contrast, bacteria that invade the periodontium appear to be less problematic so that blocking arms of the host response tend to reduce the disease process. Interestingly, both lesions of endodontic origin and periodontitis exhibit inflammation that appears to inhibit bone formation. In periodontitis, the spatial location of the inflammation is likely to be important so that a host response that is restricted to a subepithelial space is associated with gingivitis, while a host response closer to bone is linked to bone resorption and periodontitis. However, the persistence of inflammation is also thought to be important in periodontitis since inflammation present during coupled bone formation may limit the capacity to repair the resorbed bone.
Keywords: bacteria; bone; chemokine; cytokine; endodontic lesion; gingivitis; inflammation; periodontitis.
Figures



References
-
- Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol. 1965;20:340–9. - PubMed
-
- Ricucci D, Siqueira JF, Jr, Bate AL, Pitt Ford TR. Histologic investigation of root canal-treated teeth with apical periodontitis: a retrospective study from twenty-four patients. J Endod. 2009;35:493–502. - PubMed
-
- Nair PN. Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit Rev Oral Biol Med. 2004;15:348–81. - PubMed
-
- Liapatas S, Nakou M, Rontogianni D. Inflammatory infiltrate of chronic periradicular lesions: an immunohistochemical study. Int Endod J. 2003;36:464–71. - PubMed
-
- Stashenko P, Wang C, Riley E, Wu Y, Ostroff G, Niederman R. Reduction of infection-stimulated peripical bone resorption by the biological response modifier PGG glucan. J Dent Res. 1995;74:323–30. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources