

Male microchimerism in peripheral blood leukocytes from women with multiple sclerosis
- PMID: 21547029
- PMCID: PMC3084949
- DOI: 10.4161/chim.2.1.15151
Male microchimerism in peripheral blood leukocytes from women with multiple sclerosis
Abstract
Background: Fetal microchimerism (F-MC), the persistence of fetal cells in the mother, is frequently encountered following pregnancy. The high prevalence of F-MC in autoimmune disease prompts consideration of the role for immune tolerance and regulation. This study examines the association between F-MC and multiple sclerosis (MS), an autoimmune disorder, of undetermined etiology.
Results: 21 out of 51 MS-positive subjects (41%) were classified as positive for F-MC; 4 of 22 (18%) of MS-negative sibling controls, were also positive for MC (p = 0.066). Unanticipated F-MC in controls lead to re-evaluation using 30 female singleton cord blood units (CBUs) as a biological control. Four CBUs were low-level positive.
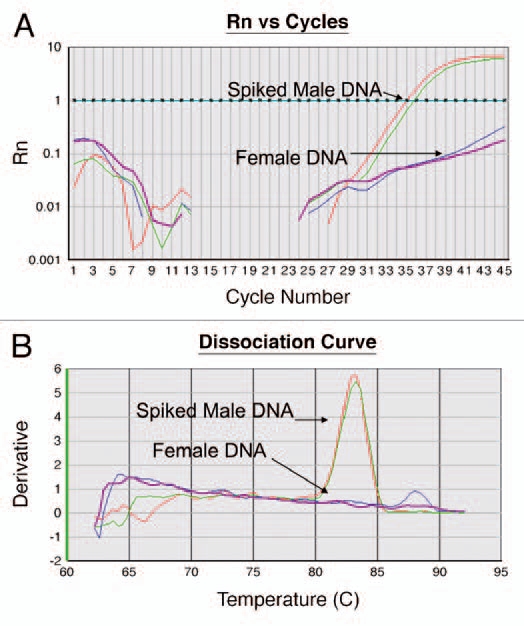
Study design and methods: Seventy-three female subjects were assigned to three groups according to disease status and pregnancy history: (1) MS positive (+) women with a history of one male pregnancy before symptom onset (n = 27); (2) MS negative (-) female siblings of MS(+) women with a history of one male pregnancy (n = 22); and (3) MS(+) women that reported never having been pregnant (n = 24). Ten micrograms of genomic DNA obtained from peripheral blood leukocytes of each subject were analyzed for F-MC using allele-specific real-time PCR targeting the SR-Y sequence on the Y-chromosome. MC classification was dichotomous (positive vs. negative) based on PCR results.
Conclusion: The association between F-MC and MS warrants further study to define this relationship. F-MC in women self-reporting as nulligravid, supports previous findings that a significant proportion of pregnancies go undetected. This lead to re-validation of a Y-chromosome based assay for F-MC detection.
Figures
Similar articles
-
Male microchimerism in peripheral blood from women with multiple sclerosis in Isfahan Province.Int J Immunogenet. 2020 Apr;47(2):175-179. doi: 10.1111/iji.12465. Epub 2019 Dec 12. Int J Immunogenet. 2020. PMID: 31833227
-
Male microchimerism at high levels in peripheral blood mononuclear cells from women with end stage renal disease before kidney transplantation.PLoS One. 2012;7(3):e32248. doi: 10.1371/journal.pone.0032248. Epub 2012 Mar 5. PLoS One. 2012. PMID: 22403639 Free PMC article.
-
Low prevalence of male microchimerism in women with Mayer-Rokitansky-Küster-Hauser syndrome.Hum Reprod. 2019 Jun 4;34(6):1117-1125. doi: 10.1093/humrep/dez044. Hum Reprod. 2019. PMID: 31111890 Free PMC article.
-
Microchimerism and stem cell transplantation in multiple sclerosis.Int Rev Neurobiol. 2007;79:173-202. doi: 10.1016/S0074-7742(07)79008-6. Int Rev Neurobiol. 2007. PMID: 17531842 Review.
-
Microchimerism in autoimmunity and transplantation: potential relevance to multiple sclerosis.J Neuroimmunol. 2002 May;126(1-2):126-33. doi: 10.1016/s0165-5728(02)00048-6. J Neuroimmunol. 2002. PMID: 12020964 Review.
Cited by
-
Statistical Methods for Unusual Count Data: Examples From Studies of Microchimerism.Am J Epidemiol. 2016 Nov 15;184(10):779-786. doi: 10.1093/aje/kww093. Am J Epidemiol. 2016. PMID: 27769989 Free PMC article.
-
Microchimerism in multiple sclerosis: The association between sex of offspring and MRI features in women with multiple sclerosis.Front Neurosci. 2023 Feb 7;17:1091955. doi: 10.3389/fnins.2023.1091955. eCollection 2023. Front Neurosci. 2023. PMID: 36824218 Free PMC article.
-
Fetal microchimeric cells in autoimmune thyroid diseases: harmful, beneficial or innocent for the thyroid gland?Chimerism. 2013 Oct-Dec;4(4):111-8. doi: 10.4161/chim.25055. Epub 2013 May 20. Chimerism. 2013. PMID: 23723083 Free PMC article. Review.
-
Advancing the detection of maternal haematopoietic microchimeric cells in fetal immune organs in mice by flow cytometry.Chimerism. 2014;5(3-4):99-102. doi: 10.4161/19381956.2014.959827. Epub 2014 Oct 30. Chimerism. 2014. PMID: 25483743 Free PMC article.
-
Fetomaternal immune cross-talk and its consequences for maternal and offspring's health.Nat Med. 2013 May;19(5):548-56. doi: 10.1038/nm.3160. Epub 2013 May 7. Nat Med. 2013. PMID: 23652115 Review.
References
-
- Steinman L, Martin R, Bernard C, Conlon P, Oksenberg JR. Multiple sclerosis: deeper understanding of its pathogenesis reveals new targets for therapy. Annu Rev Neurosci. 2002;25:491–505. - PubMed
-
- Murray TJ. The history of multiple sclerosis: the changing frame of the disease over the centuries. J Neurol Sci. 2009;277:3–8. - PubMed
-
- Chaudhuri A, Behan PO. Multiple sclerosis is not an autoimmune disease. Arch Neurol. 2004;61:1610–1612. - PubMed
-
- Weiner HL. Multiple sclerosis is an inflammatory T-cell-mediated autoimmune disease. Arch Neurol. 2004;61:1613–1615. - PubMed
-
- Racke MK, Lovett-Racke AE, Karandikar NJ. The mechanism of action of glatiramer acetate treatment in multiple sclerosis. Neurology. 2010;74:25–30. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials