

Erythrocytapheresis: Do Not Forget a Useful Therapy!
- PMID: 21547107
- PMCID: PMC3083277
- DOI: 10.1159/000112044
Erythrocytapheresis: Do Not Forget a Useful Therapy!
Abstract
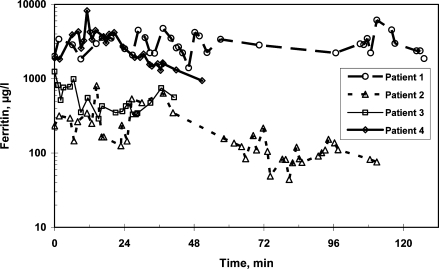
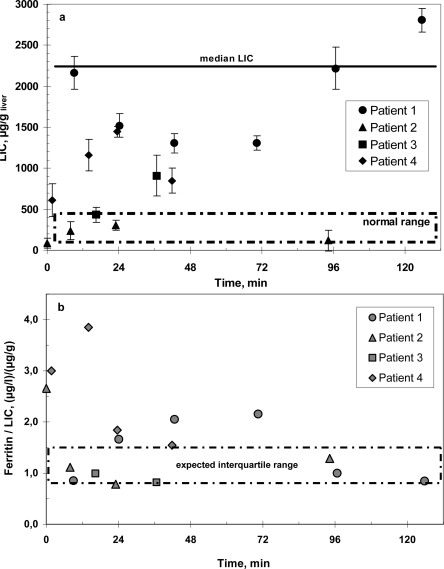
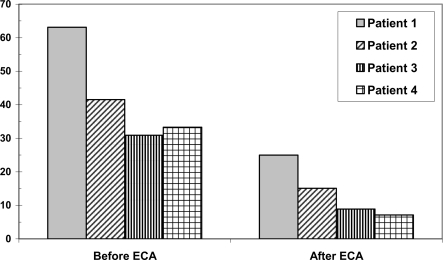
SUMMARY: In patients with pathologically altered erythrocytes, red blood cell exchange is a very efficient therapeutic measure without important side effects. With increasing migration more patients with e.g. severe malaria or sickle cell anemia have to be treated. In minor or bidirectional ABO-mismatched stem cell transplantations after reduced intensity conditioning, hemolysis can be prevented by prophylactic erythrocytapheresis. Other rare indications for red blood cell exchange are advanced erythropoietic protoporphyria and babesiosis. Sickle cell anemia can be treated with hydroxyurea. Transfusions are administered when necessary, but this results in iron overload in the long term. An expensive but safe and very efficient treatment alternative is red blood cell exchange. In cases with stroke, acute chest syndrome and other severe complications, erythrocytapheresis reproducibly breaks the vicious circle of sickling and increasing oxygen deficiency. At the same time one can aim at an exact end hematocrit. In severe malaria, erythrocytapheresis both reduces parasite load to the designated extent and reconstitutes reduced oxygen transport capacity without serious adverse effects. Here we describe our experience of erythrocytapheresis in long-term prophylaxis of complications in sickle cell anemia and sickle cell thalassemia patients. The documentation of improved iron balance was carried out by liver susceptometry.
Zusammenfassung: Die Erythrozytapherese ist eine sehr effiziente therapeutische Maßnahme bei Patienten mit klinischen Problemen durch pathologisch veränderte Erythrozyten. Durch zunehmende Migration und Reisen wird es immer häufiger nötig, schwere Malaria sowie Patienten mit Sichelzellanämie und Thalassämie zu behandeln. Sichelzellanämie wird bei Bedarf mit Hydroxyurea behandelt, um die Hämoglobin-F-Konzentration im Blut zu steigern. Transfusionen werden bei Hypoxie und schwerer Anämie verabreicht, aber dadurch entsteht eine Eisenüberladung. In der Zulassung befindliche orale Chelatbildner sollen dieses Problem verringern. Eine teure, aber nebenwirkungsarme und sichere Alternative ist die Erythrozytapherese. Bei Patienten mit Schlaganfall, akutem Thoraxsyndrom und anderen schweren Sichelzellkomplikationen führt der Erythrozytenaustausch zu einer schnellen und reproduzierbaren Besserung; der Teufelskreis zwischen Sichelzellbildung, Minderdurchblutung und Hypoxämie wird gebrochen und der gewünschte Hämatokrit kann erzielt werden. Bei den meisten Malariapatienten ist medikamentöse Therapie ausreichend, aber bei starkem Parasitenbefall können Hämolyse und Anämie prompt und nebenwirkungsarm durch Erythrozytenaustausch behoben werden; die Menge befallener Erythrozyten wird in den angepeilten Bereich bewegt und der Patient wird einer Medikamententherapie zugänglich. Wir beschreiben unsere Erfahrungen in der Sekundärprophylaxe von Komplikationen bei Sichelzellanämie und Sichelzellthalassämie. Der Schutz vor Eisenüberladung wurde mit Hilfe der Leber-Biosuszeptometrie dokumentiert.
Figures
References
-
- Thurston GB, Henderson NM, Jeng M. Effects of erythrocytapheresis transfusion on the viscoelasticity of sickle cell blood. Clin Hemorheol Microcirc. 2004;30:83–97. - PubMed
-
- Adams HP, Jr, Adams RJ, Brott T, del Zoppo GJ, Furlan A, Goldstein LB, Grubb RL, Higashida R, Kidwell C, Kwiatkowski TG, Marler JR, Hademenos GJ. Guidelines for the early management of patients with ischemic stroke: a scientific statement from the Stroke Council of the American Stroke Association. Stroke. 2003;34:1056–1083. - PubMed
-
- Swerdlow PS. Red cell exchange in sickle cell disease. Hematology Am Soc Hematol Educ Program. 2006:48–53. - PubMed
-
- Adams RJ, Brambilla D. Discontinuing prophylactic transfusions used to prevent stroke in sickle cell disease. N Engl J Med. 2005;353:2769–2778. - PubMed
-
- Adams RJ. Lessons from the Stroke Prevention Trial in Sickle Cell Anemia (STOP) study. J Child Neurol. 2000;15:344–349. - PubMed
LinkOut - more resources
Full Text Sources
