

Assessment of patient doses in CR examinations throughout a large health region
- PMID: 21547516
- PMCID: PMC3264727
- DOI: 10.1007/s10278-011-9390-1
Assessment of patient doses in CR examinations throughout a large health region
Abstract
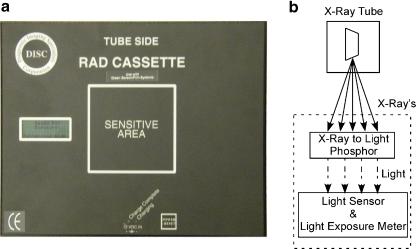
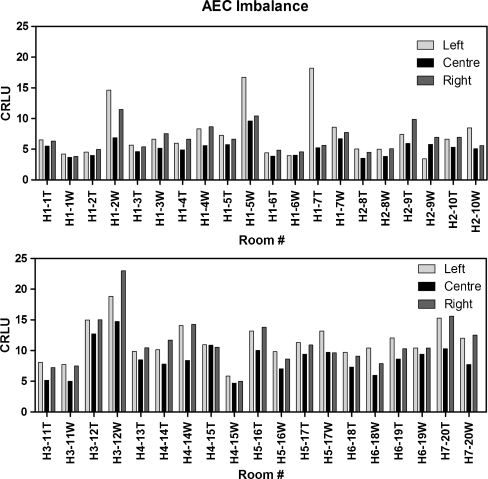
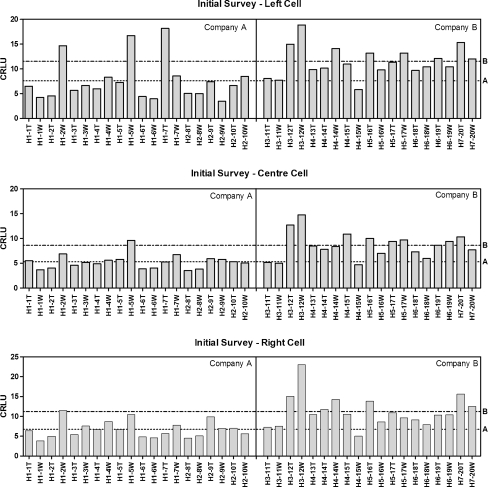
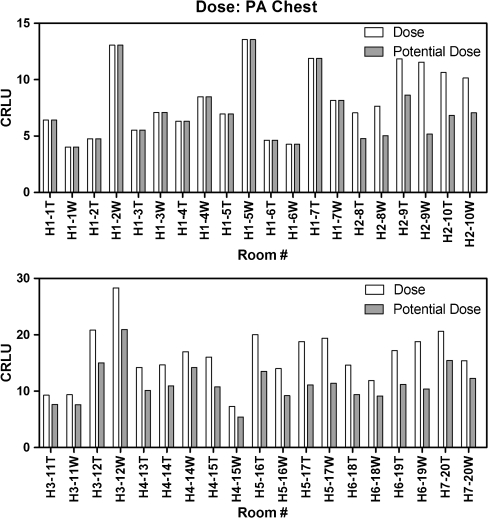
Optimization and standardization of radiographic procedures in a health region minimizes patient exposure while producing diagnostic images. This report highlights the dose variation in common computed radiography (CR) examinations throughout a large health region. The RadChex cassette was used to measure the radiation exposure at the table or wall bucky in 20 CR rooms, in seven hospitals, using CR technology from two vendors. Exposures were made to simulate patient exposure (21 cm polymethyl methacrylate) under standard conditions for each bucky: 81 kVp at 100 cm for anteroposterior abdomen table bucky exposures (180 cm for posteroanterior chest wall bucky exposures), using the left, the right, or the center automatic exposure control (AEC) cells. Protocol settings were recorded. An average of 37% variation was found between AEC chambers, with a range between 4% and 137%. A 60% difference in dose was discovered between manufacturers, which was the result of the manufacture's image processing algorithm and subsequently corrected via software updates. Finally, standardizing AEC cell selection during common chest examinations could reduce patient dose by up to 30%. In a large health region, variation in exam protocols can occur, leading to unnecessary patient dose from the same type of examination. Quality control programs must monitor exam protocols and AEC chamber calibration in CR to ensure consistent, minimal, patient dose, regardless of hospital or CR vendor. Furthermore, this report highlights the need for communication between radiologists, technologists, medical physicist, service engineers, and manufacturers required to optimize CR protocols.
Figures
References
-
- Berni D, Gori C, Lazzari B, Mazzocchi S, Rossi F, Zatelli G. Use of TLD in evaluating diagnostic reference levels for some radiological examinations. Radiat Prot Dosimetry. 2002;101:411–413. - PubMed
-
- Bacher K, Smeets P, Bonnarens K, DeHauwere A, Verstraete K, Thierens H. Dose reduction in patients undergoing chest imaging: digital amorphous silicon flat-panel detector versus conventional film-screen radiography and phosphor-based computed radiography. Am J Roentgenology. 2003;181:923–929. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
