

A tissue-engineered muscle repair construct for functional restoration of an irrecoverable muscle injury in a murine model
- PMID: 21548710
- PMCID: PMC3161107
- DOI: 10.1089/ten.TEA.2010.0682
A tissue-engineered muscle repair construct for functional restoration of an irrecoverable muscle injury in a murine model
Abstract
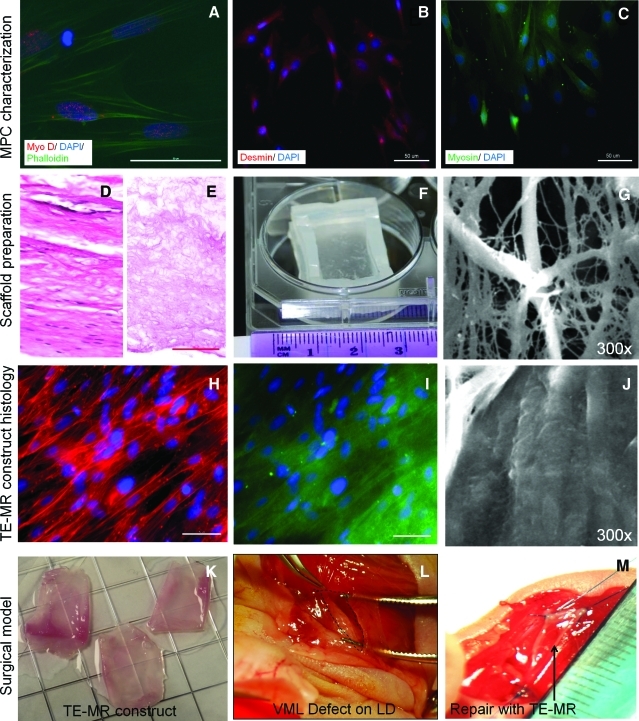
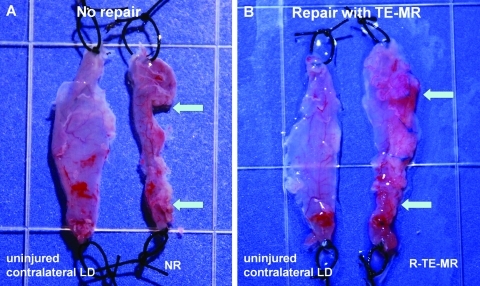
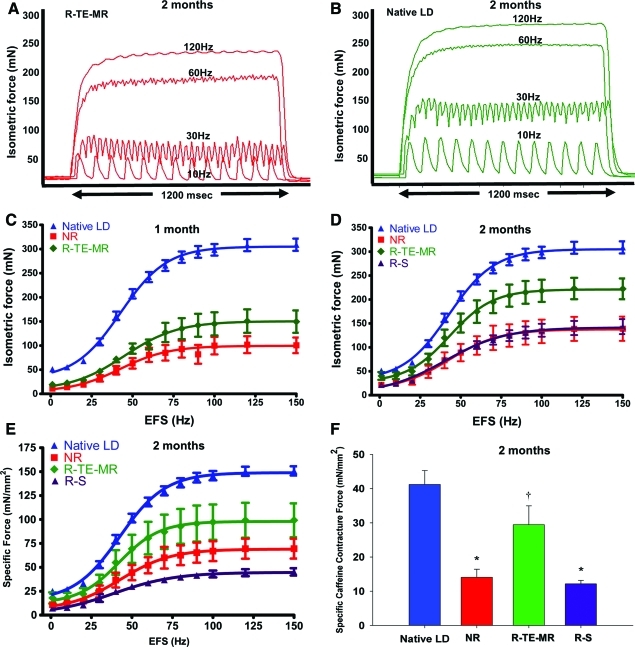
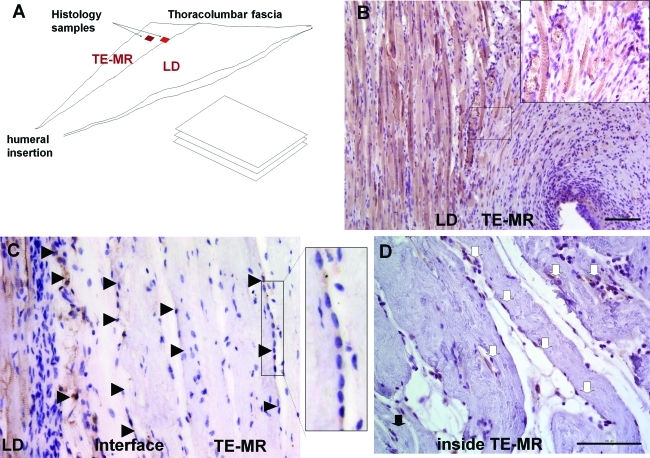
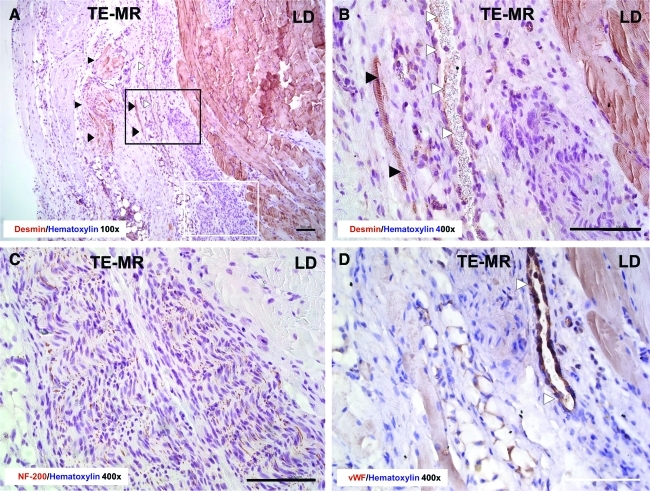
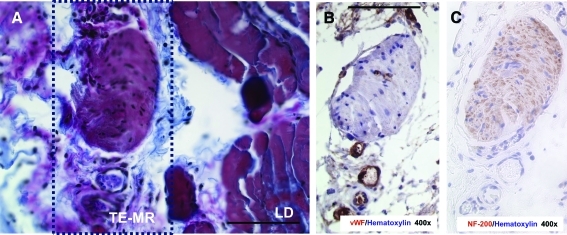
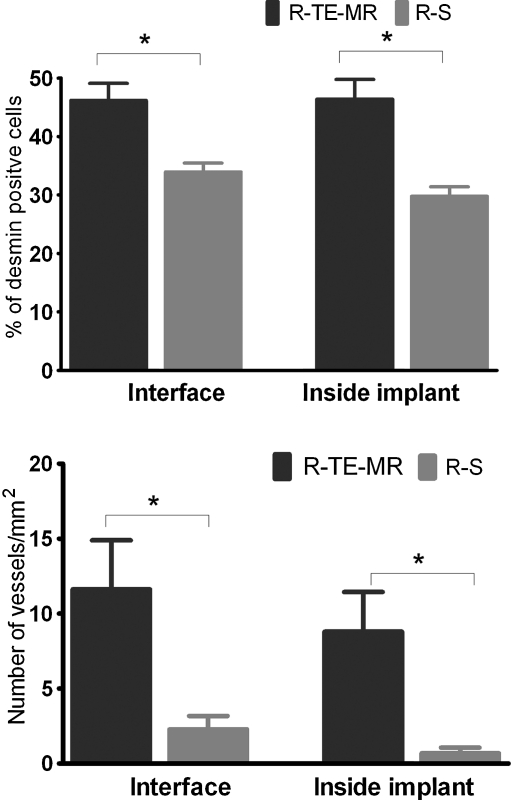
There are no effective clinical treatments for volumetric muscle loss (VML) resulting from traumatic injury, tumor excision, or other degenerative diseases of skeletal muscle. The goal of this study was to develop and characterize a more clinically relevant tissue-engineered muscle repair (TE-MR) construct for functional restoration of a VML injury in the mouse lattissimus dorsi (LD) muscle. To this end, TE-MR constructs developed by seeding rat myoblasts on porcine bladder acellular matrix were preconditioned in a bioreactor for 1 week and implanted in nude mice at the site of a VML injury created by excising 50% of the native LD. Two months postinjury and implantation of TE-MR, maximal tetanic force was ∼72% of that observed in native LD muscle. In contrast, injured LD muscles that were not repaired, or were repaired with scaffold alone, produced only ∼50% of native LD muscle force after 2 months. Histological analyses of LD tissue retrieved 2 months after implantation demonstrated remodeling of the TE-MR construct as well as the presence of desmin-positive myofibers, blood vessels, and neurovascular bundles within the TE-MR construct. Overall, these encouraging initial observations document significant functional recovery within 2 months of implantation of TE-MR constructs and provide clear proof of concept for the applicability of this technology in a murine VML injury model.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
