

Provider perceptions of barriers to the emergency use of tPA for acute ischemic stroke: a qualitative study
- PMID: 21548943
- PMCID: PMC3112102
- DOI: 10.1186/1471-227X-11-5
Provider perceptions of barriers to the emergency use of tPA for acute ischemic stroke: a qualitative study
Abstract
Background: Only 1-3% of ischemic stroke patients receive thrombolytic therapy. Provider barriers to adhering with guidelines recommending tPA delivery in acute stroke are not well known. The main objective of this study was to describe barriers to thrombolytic use in acute stroke care.
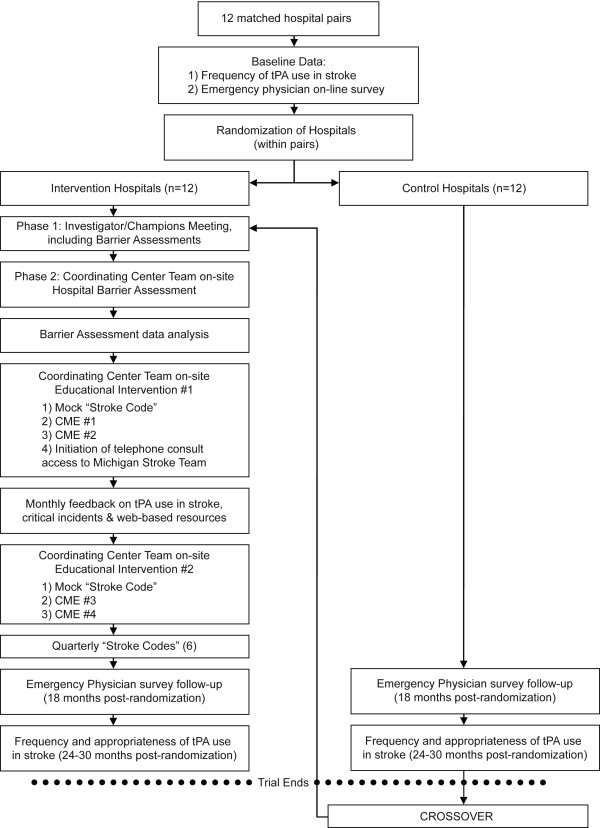
Methods: Twenty-four hospitals were randomly selected and matched into 12 pairs. Barrier assessment occurred at intervention sites only, and utilized focus groups and structured interviews. A pre-specified taxonomy was employed to characterize barriers. Two investigators independently assigned themes to transcribed responses. Seven facilitators (three emergency physicians, two nurses, and two study coordinators) conducted focus groups and interviews of emergency physicians (65), nurses (62), neurologists (15), radiologists (12), hospital administrators (12), and three others (hospitalists and pharmacist).
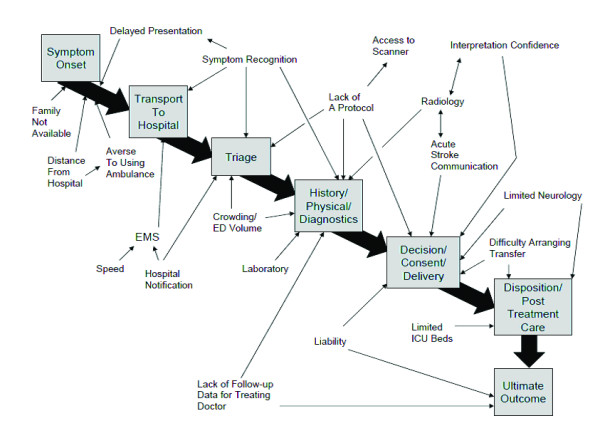
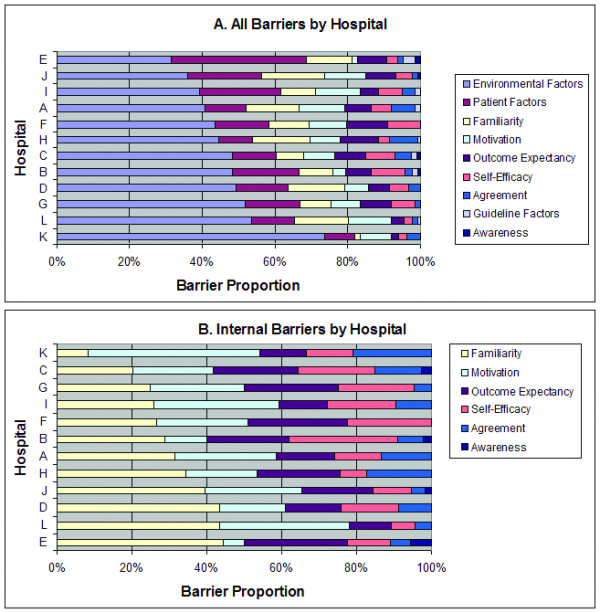
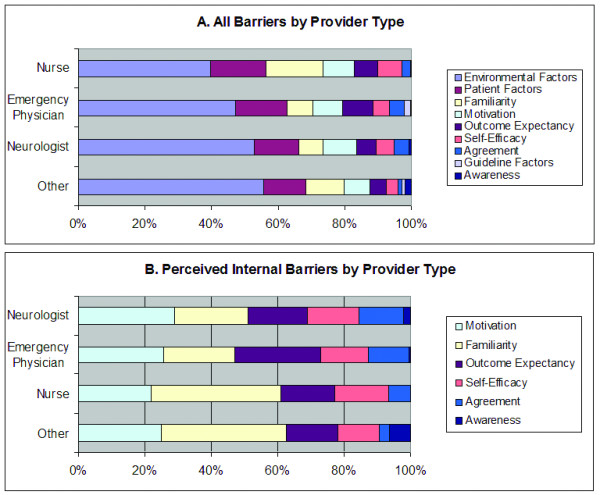
Results: The following themes represented the most important external barriers: environmental and patient factors. Important barriers internal to the clinician included familiarity with and motivation to adhere to the guidelines, lack of self-efficacy and outcome expectancy. The following themes were not substantial barriers: lack of awareness of the existence of acute stroke guidelines, presence of conflicting guidelines, and lack of agreement with the guidelines.
Conclusions: Healthcare providers perceive environmental and patient-related factors as the primary barriers to adherence with acute stroke treatment guidelines. Interventions focused on increasing physician familiarity with and motivation to follow guidelines may be of highest yield in improving adherence. Improving self-efficacy in performing guideline concordant care may also be useful.
Trial registration: ClinicalTrials.gov NCT00349479.
Figures
References
-
- Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, Hailpern SM, Ho M, Howard V, Kissela B, Kittner S, Lloyd-Jones D, McDermott M, Meigs J, Moy C, Nichol G, O'Donnell C, Roger V, Sorlie P, Steinberger J, Thom T, Wilson M, Hong Y. Committee ftAHAS, Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics--2008 Update: A Report From the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117(4):e25–146. - PubMed
-
- Adams HP Jr, del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, Grubb RL, Higashida RT, Jauch EC, Kidwell C, Lyden PD, Morgenstern LB, Qureshi AI, Rosenwasser RH, Scott PA, Wijdicks EFM. Guidelines for the Early Management of Adults With Ischemic Stroke: A Guideline From the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007;38(5):1655–1711. doi: 10.1161/STROKEAHA.107.181486. - DOI - PubMed
-
- del Zoppo GJ, Saver JL, Jauch EC, Adams HP, Jr, on behalf of the American Heart Association Stroke Council. Expansion of the Time Window for Treatment of Acute Ischemic Stroke With Intravenous Tissue Plasminogen Activator. A Science Advisory From the American Heart Association/American Stroke Association. Stroke. 2009. STROKEAHA.109.192535. - PMC - PubMed
-
- Barber PA, Zhang J, Demchuk AM, Hill MD, Buchan AM. Why are stroke patients excluded from TPA therapy?: An analysis of patient eligibility. Neurology. 2001;56(8):1015–1020. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
