

High-normal albuminuria and risk of heart failure in the community
- PMID: 21549463
- PMCID: PMC3119712
- DOI: 10.1053/j.ajkd.2011.02.391
High-normal albuminuria and risk of heart failure in the community
Abstract
Background: Albuminuria has been associated with cardiovascular risk, but the relationship of high-normal albuminuria to subsequent heart failure has not been well established.
Study design: Prospective observational study, the Atherosclerosis Risk in Communities (ARIC) Study.
Setting & participants: 10,975 individuals free from heart failure were followed up from the fourth ARIC Study visit (1996-1998) through January 2006.
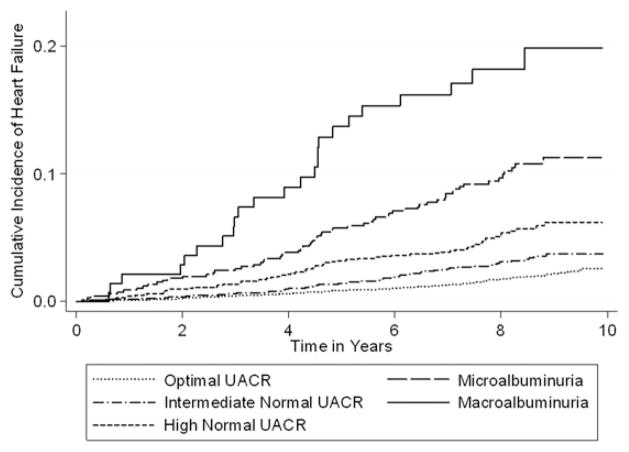
Predictor: Urinary albumin-creatinine ratio (UACR), analyzed continuously and categorically as optimal (<5 mg/g), intermediate-normal (5-9 mg/g), high-normal (10-29 mg/g), microalbuminuria (30-299 mg/g), and macroalbuminuria (≥300 mg/g).
Outcomes & measurements: Incident heart failure was defined as a heart failure-related hospitalization or death. Cox proportional hazard models were used to calculate the HR of heart failure after adjustment for age, race, sex, estimated glomerular filtration rate (eGFR), and other cardiovascular risk factors.
Results: Individuals were followed up for a median of 8.3 years and experienced 344 heart failure events. Compared with normal UACR, albuminuria was associated with a progressively increased risk of heart failure from intermediate-normal (adjusted HR, 1.54; 95% CI, 1.12-2.11) and high-normal UACR (adjusted HR, 1.91; 95% CI, 1.38-2.66) to microalbuminuria (adjusted HR, 2.49; 95% CI, 1.77-3.50) and macroalbuminuria (adjusted HR, 3.47; 95% CI, 2.10-5.72). Results were similar in secondary analyses of participants censored at the time of coronary heart disease event and along a range of eGFRs.
Limitations: UACR was measured as a single random sample.
Conclusions: Albuminuria is associated with subsequent heart failure, even in individuals with few cardiovascular risk factors and UACR within the normal range. Our results suggest that the association between albuminuria and heart failure may not be mediated fully by ischemic heart disease or kidney disease, measured using eGFR.
Copyright © 2011 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- National Kidney Foundation. K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 suppl 1):S1–266. - PubMed
-
- Deckert T, Feldt-Rasmussen B, Borch-Johnsen K, Jensen T, Kofoed-Enevoldsen A. Albuminuria reflects widespread vascular damage. The Steno hypothesis. Diabetologia. 1989;32(4):219–226. - PubMed
-
- Dobre D, Nimade S, de Zeeuw D. Albuminuria in heart failure: what do we really know? Curr Opin Cardiol. 2009;24(2):148–154. - PubMed
-
- Lamb EJ, MacKenzie F, Stevens PE. How should proteinuria be detected and measured? Ann Clin Biochem. 2009;46(pt 3):205–217. - PubMed
-
- Danziger J. Importance of low-grade albuminuria. Mayo Clin Proc. 2008;83(7):806–812. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC055016/HL/NHLBI NIH HHS/United States
- N01 HC055019/HL/NHLBI NIH HHS/United States
- N01-HC-55016/HC/NHLBI NIH HHS/United States
- N01-HC-55021/HC/NHLBI NIH HHS/United States
- N01 HC055020/HL/NHLBI NIH HHS/United States
- N01-HC-55019/HC/NHLBI NIH HHS/United States
- N01-HC-55015/HC/NHLBI NIH HHS/United States
- 5T32HL007024/HL/NHLBI NIH HHS/United States
- N01-HC-55020/HC/NHLBI NIH HHS/United States
- N01 HC055022/HL/NHLBI NIH HHS/United States
- N01-HC-55018/HC/NHLBI NIH HHS/United States
- N01-HC-55022/HC/NHLBI NIH HHS/United States
- N01 HC055021/HL/NHLBI NIH HHS/United States
- T32 HL007024/HL/NHLBI NIH HHS/United States
- N01 HC055015/HL/NHLBI NIH HHS/United States
- N01 HC055018/HL/NHLBI NIH HHS/United States
- K08 HS023683/HS/AHRQ HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
