

The potential use of 2-[¹⁸F]fluoro-2-deoxy-D-galactose as a PET/CT tracer for detection of hepatocellular carcinoma
- PMID: 21553087
- PMCID: PMC3152607
- DOI: 10.1007/s00259-011-1831-z
The potential use of 2-[¹⁸F]fluoro-2-deoxy-D-galactose as a PET/CT tracer for detection of hepatocellular carcinoma
Abstract
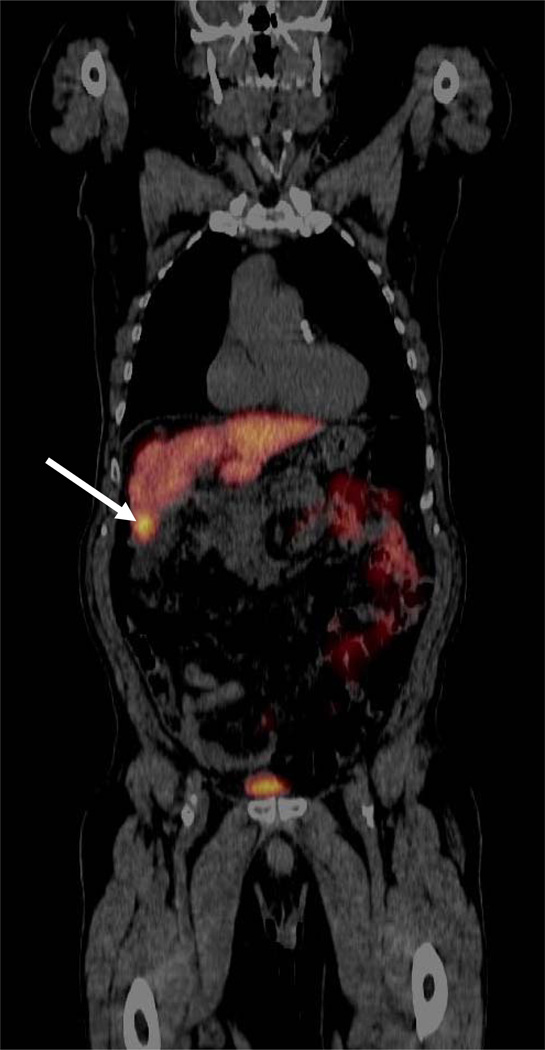
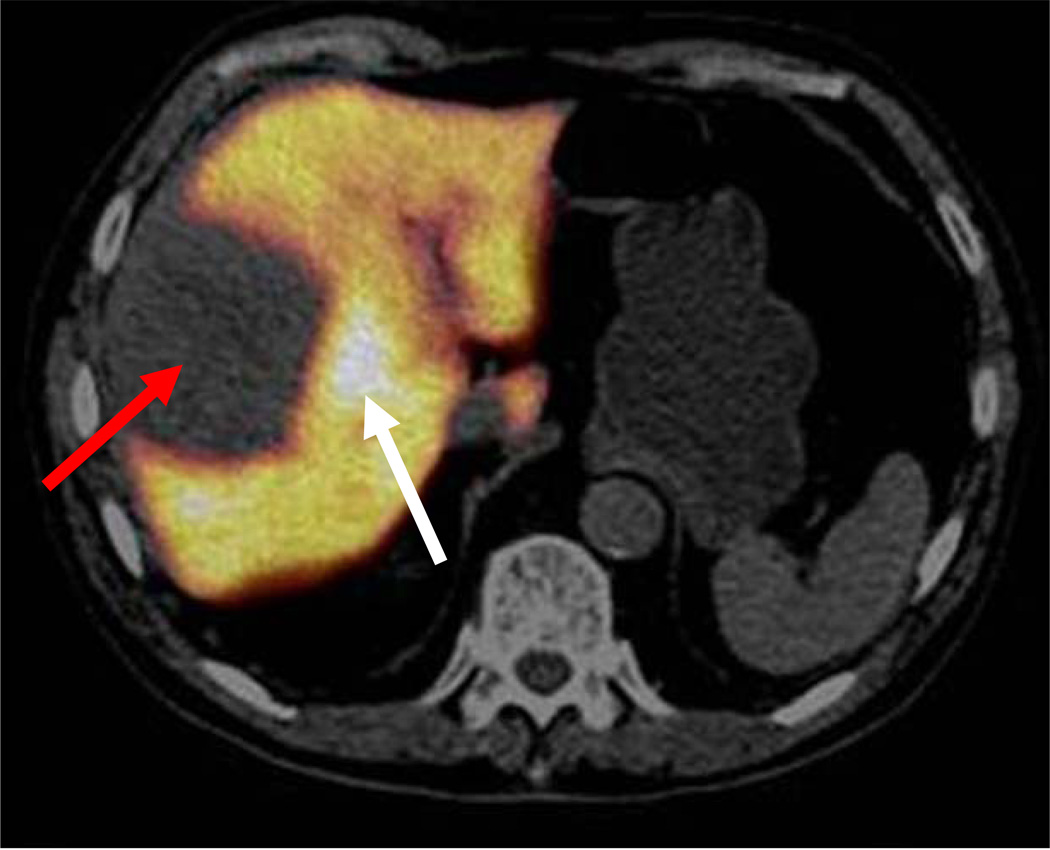
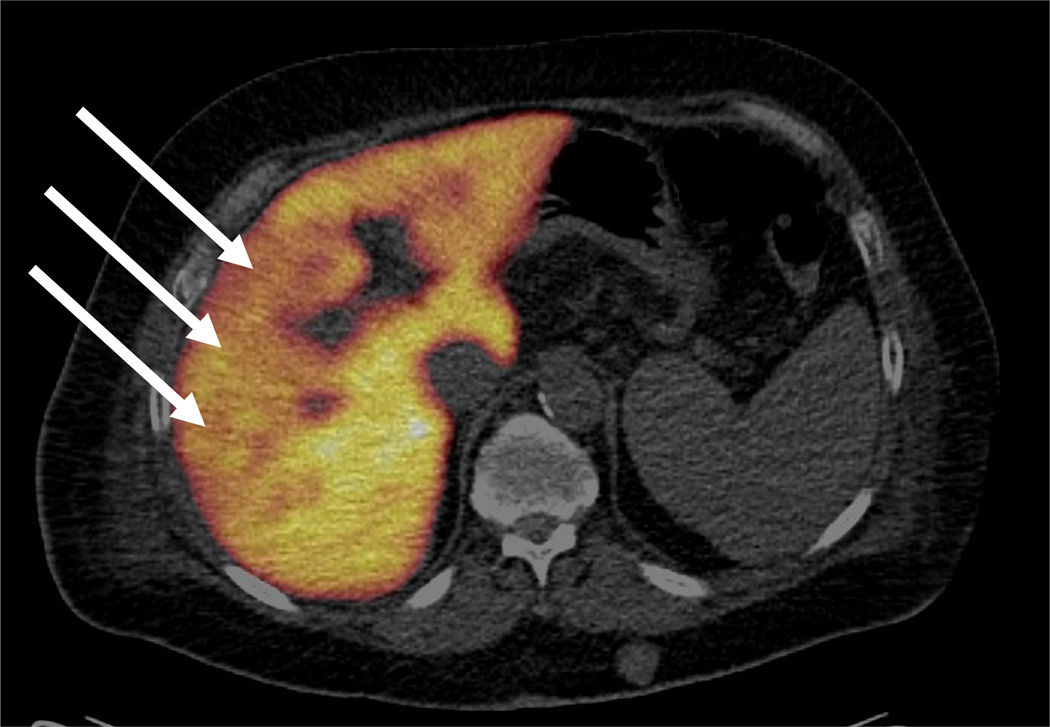
Purpose: The aim of the study was to evaluate the feasibility of using the hepatocyte-specific positron emission tomography (PET) tracer 2-[(18)F]fluoro-2-deoxy-D-galactose (FDGal) as a tracer for hepatocellular carcinoma (HCC).
Methods: In addition to standard clinical investigations, 39 patients with known HCC or suspected of having HCC underwent a partial-body FDGal PET/CT (from base of skull to mid-thigh). Diagnosis of HCC was based on internationally approved criteria. FDGal PET/CT images were analysed for areas with high (hot spots) or low (cold spots) tracer accumulation when compared to surrounding tissue.
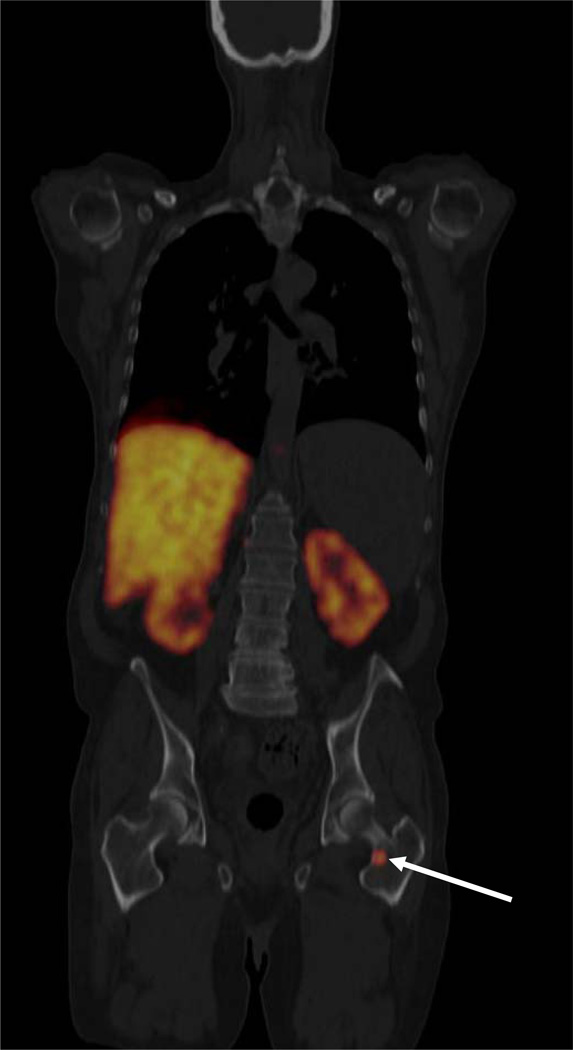
Results: Seven patients did not have HCC and FDGal PET/CT was negative in each of them. Twenty-three patients had HCC and were included before treatment. FDGal PET/CT correctly identified 22 of these patients, which was comparable to contrast-enhanced CT. Interestingly, FDGal PET/CT was conclusive in 12 patients in whom conventional imaging techniques were inconclusive and required additional diagnostic investigations or close follow-up. Nine patients were included after treatment of HCC and in these patients FDGal PET/CT was able to distinguish between viable tumour tissue as hot spots and areas with low metabolic activity as cold spots. FDGal PET/CT detected extrahepatic disease in nine patients which was a novel finding in eight patients.
Conclusion: FDGal PET/CT has great clinical potential as a PET tracer for detection of extra- but also intrahepatic HCC. In the present study, the specificity of FDGal PET/CT was 100%, which is very promising but needs to be confirmed in a larger, prospective study.
Conflict of interest statement
Figures
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Llovet JM, Burroughs A, Bruix J. Hepatocellular carcinoma. Lancet. 2003;362:1907–1917. - PubMed
-
- Llovet JM, Bruix J. Novel advancements in the management of hepatocellular carcinoma in 2008. J Hepatol. 2008;48:S20–S37. - PubMed
-
- Forner A, Vilana R, Ayuso C, Bianchi L, Solé M, Ayuso JR, et al. Diagnosis of hepatic nodules 20 mm or smaller in cirrhosis: prospective validation of the noninvasive diagnostic criteria for hepatocellular Carcinoma. Hepatology. 2007;47:97–104. - PubMed
-
- Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, Burroughs AK, et al. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. J Hepatol. 2001;35:421–430. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
