

Brace technology thematic series - The Sforzesco and Sibilla braces, and the SPoRT (Symmetric, Patient oriented, Rigid, Three-dimensional, active) concept
- PMID: 21554719
- PMCID: PMC3115908
- DOI: 10.1186/1748-7161-6-8
Brace technology thematic series - The Sforzesco and Sibilla braces, and the SPoRT (Symmetric, Patient oriented, Rigid, Three-dimensional, active) concept
Abstract
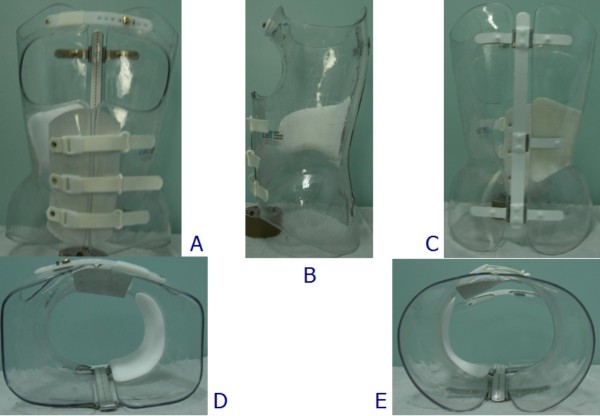
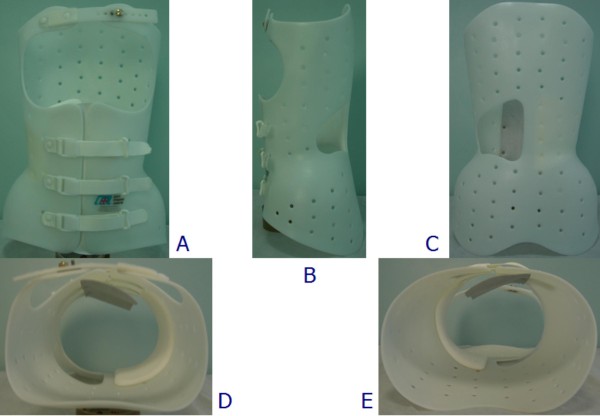
Background: Bracing is an effective strategy for scoliosis treatment, but there is no consensus on the best type of brace, nor on the way in which it should act on the spine to achieve good correction. The aim of this paper is to present the family of SPoRT (Symmetric, Patient-oriented, Rigid, Three-dimensional, active) braces: Sforzesco (the first introduced), Sibilla and Lapadula.
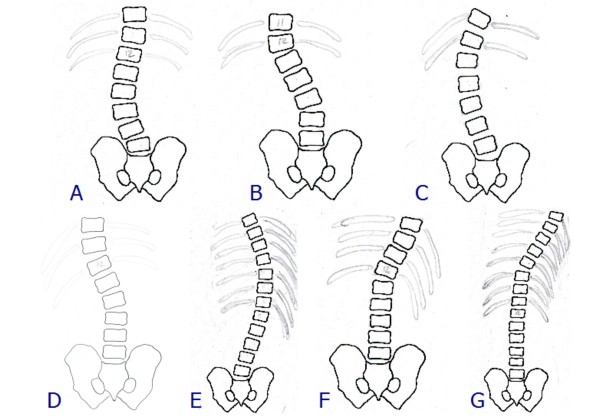
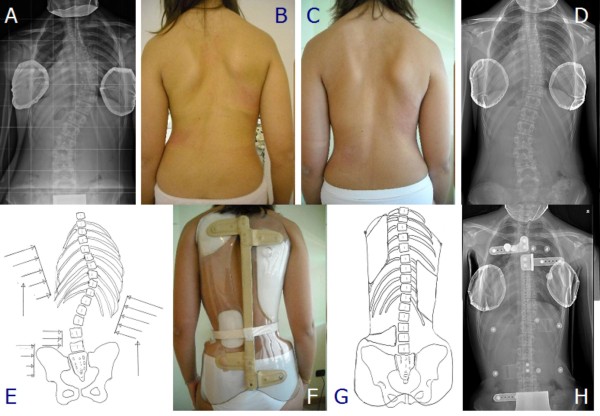
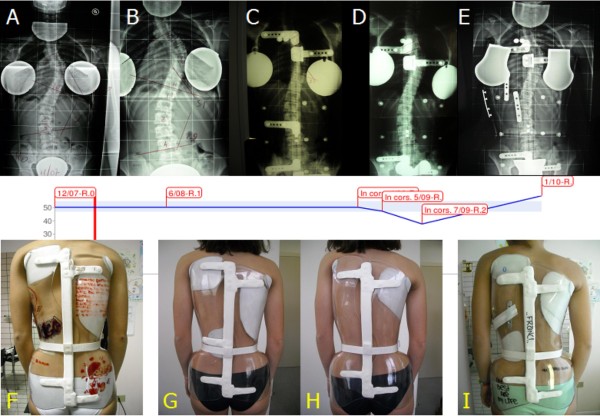
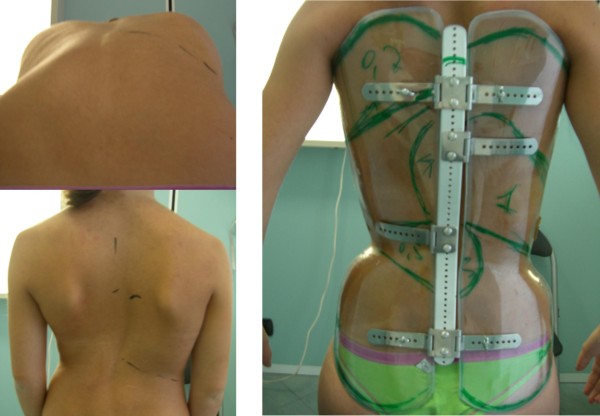
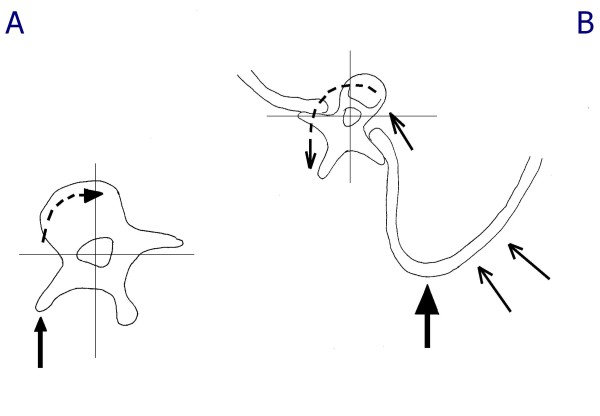
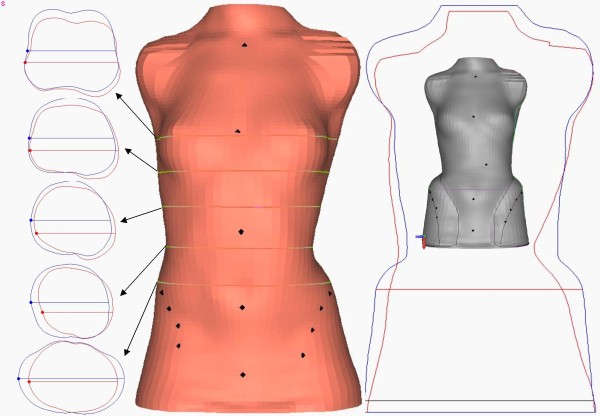
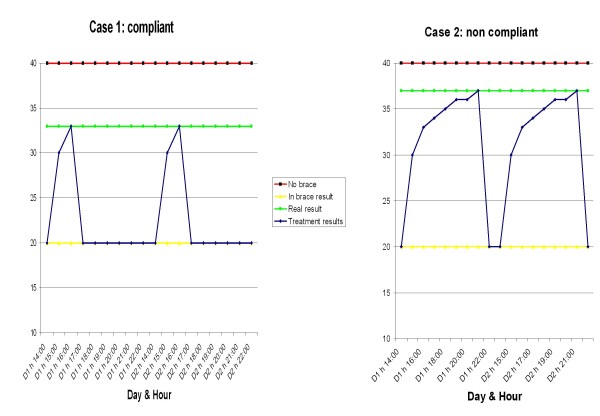
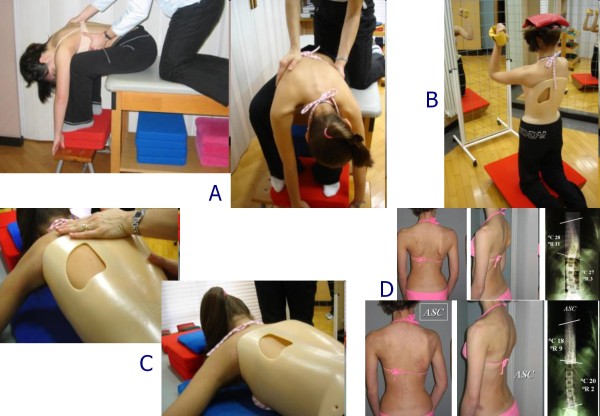
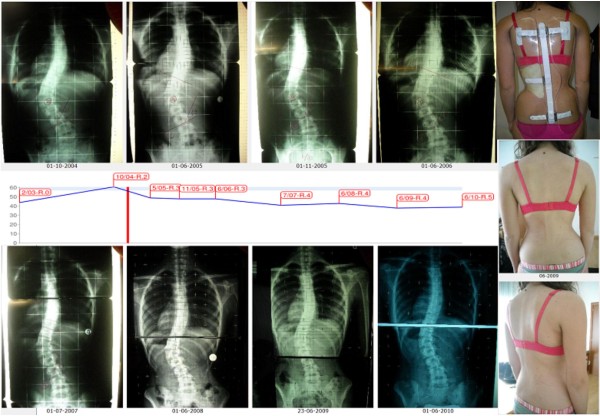
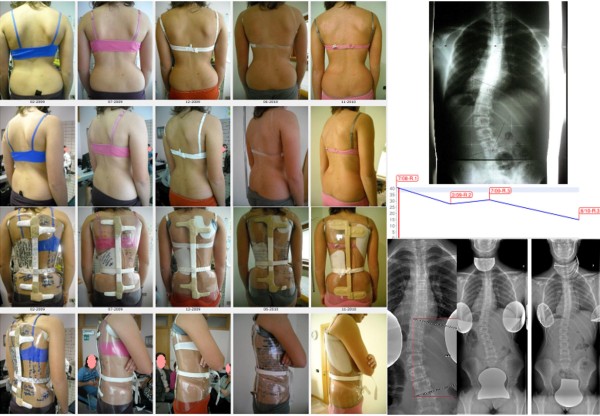
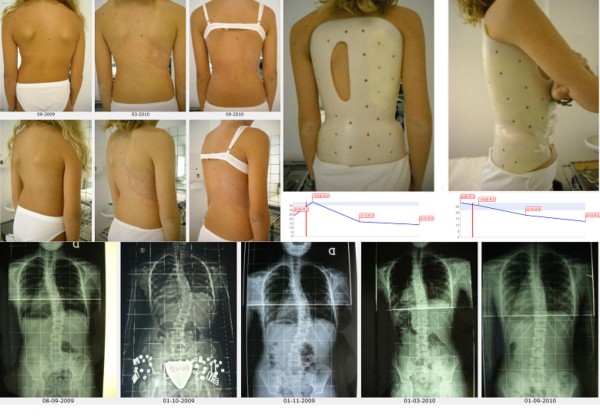
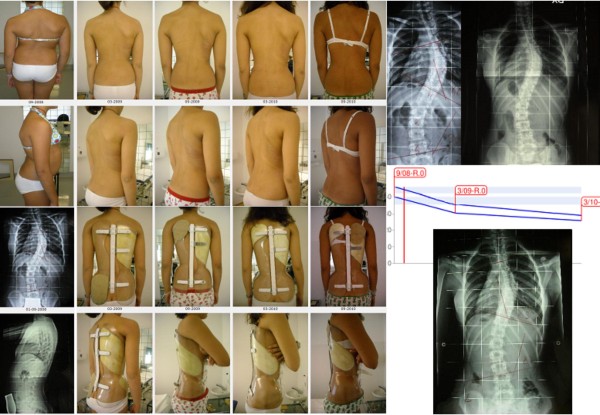
Methods: The Sforzesco brace was developed following specific principles of correction. Due to its overall symmetry, the brace provides space over pathological depressions and pushes over elevations. Correction is reached through construction of the envelope, pushes, escapes, stops, and drivers. The real novelty is the drivers, introduced for the first time with the Sforzesco brace; they allow to achieve the main action of the brace: a three-dimensional elongation pushing the spine in a down-up direction.Brace prescription is made plane by plane: frontal (on the "slopes", another novelty of this concept, i.e. the laterally flexed sections of the spine), horizontal, and sagittal. The brace is built modelling the trunk shape obtained either by a plaster cast mould or by CAD-CAM construction. Brace checking is essential, since SPoRT braces are adjustable and customisable according to each individual curve pattern.Treatment time and duration is individually tailored (18-23 hours per day until Risser 3, then gradual reduction). SEAS (Scientific Exercises Approach to Scoliosis) exercises are a key factor to achieve success.
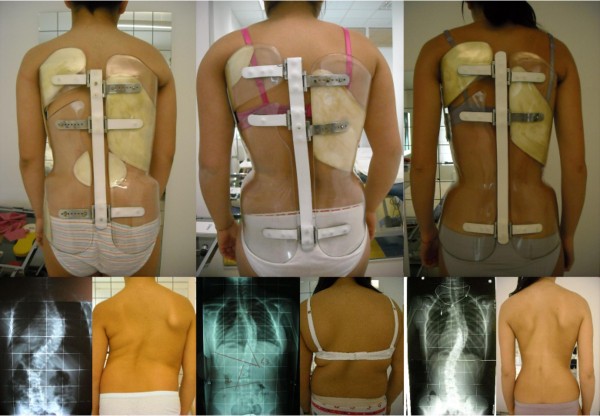
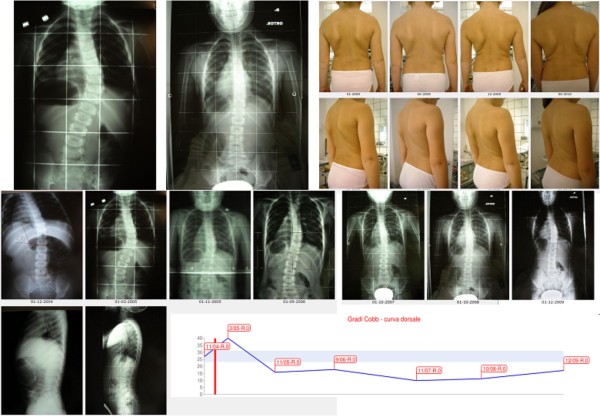
Results: The Sforzesco brace has shown to be more effective than the Lyon brace (matched case/control), equally effective as the Risser plaster cast (prospective cohort with retrospective controls), more effective than the Risser cast + Lyon brace in treating curves over 45 degrees Cobb (prospective cohort), and is able to improve aesthetic appearance (prospective cohort).
Conclusions: The SPoRT concept of bracing (three-dimensional elongation pushing in a down-up direction) is different from the other corrective systems: 3-point, traction, postural, and movement-based. The Sforzesco brace, being comparable to casting, may be the best brace for the worst cases.
Figures






References
-
- Negrini S, Minozzi S, Bettany-Saltikov J, Zaina F, Chockalingam N, Grivas TB, Kotwicki T, Maruyama T, Romano M, Vasiliadis ES. Braces for idiopathic scoliosis in adolescents. Cochrane Database Syst Rev. 2010. p. CD006850. - PubMed
-
- Negrini S, Minozzi S, Bettany-Saltikov J, Zaina F, Chockalingam N, Grivas TB, Kotwicki T, Maruyama T, Romano M, Vasiliadis ES. Braces for idiopathic scoliosis in adolescents. Spine (Phila Pa 1976) 2010;35(13):1285–1293. - PubMed
-
- Landauer F, Wimmer C, Behensky H. Estimating the final outcome of brace treatment for idiopathic thoracic scoliosis at 6-month follow-up. Pediatr Rehabil. 2003;6(3-4):201–207. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
